European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2025: post-resuscitation care
Jerry P. Nolan, Claudio Sandroni, Alain Cariou, et al
Intensive Care Med (2025)
https://doi.org/10.1007/s00134-025-08117-3
Abstract
The European Resuscitation Council (ERC) and the European Society of Intensive Care Medicine (ESICM) have collaborated to produce these post-resuscitation care guidelines for adults, which are based on the International Consensus on Cardiopulmonary Resuscitation Science with Treatment Recommendations (CoSTR) pubished by the International Liaison Committee on Resuscitation (ILCOR). The topics covered include the post-cardiac arrest syndrome, diagnosis of cause of cardiac arrest, control of oxygenation and ventilation, coronary reperfusion, haemodynamic monitoring and management, control of seizures, temperature control, general intensive care management, prognostication, long-term outcome, rehabilitation, and organ donation. The post-resuscitation care of children is described in the ERC guidelines 2025 Paediatric Life Support.
Table 1 Comparison of ERC-ESICM Post-Resuscitation Care Guidelines (2021 vs 2025)
| Topic | 2021 Guidelines | 2025 Guidelines |
|---|---|---|
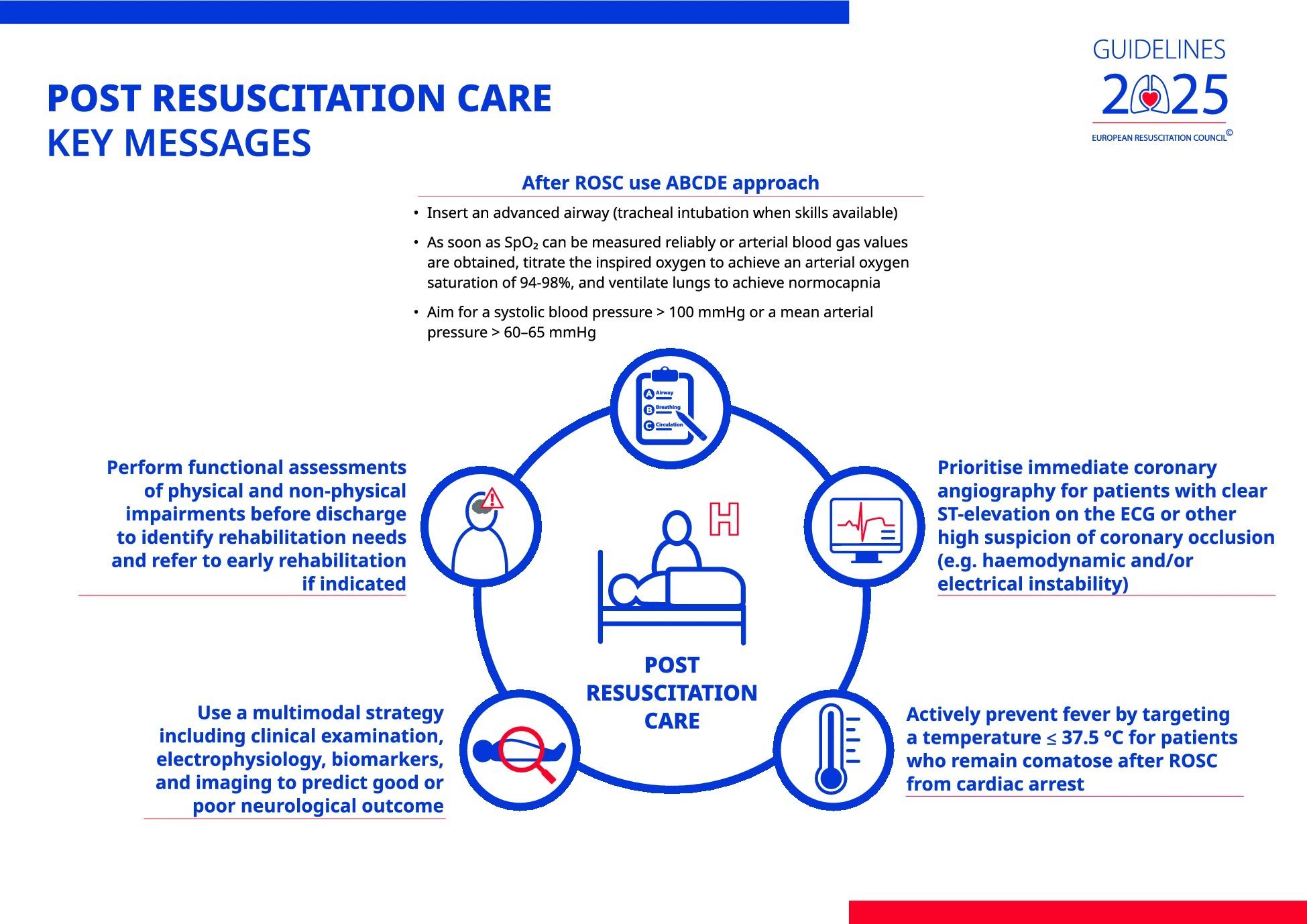
| Diagnosis of Cause and Complications of Cardiac Arrest | Suggested coronary angiography first in patients with myocardial ischemia. CT brain and chest scan were considered if coronary angiography did not find causative lesions | Coronary angiography remains first if ST-elevation is present; otherwise, dual-phase, whole-body CT scan (including head, neck, chest, abdomen, pelvis, and CT pulmonary angiography) takes priority |
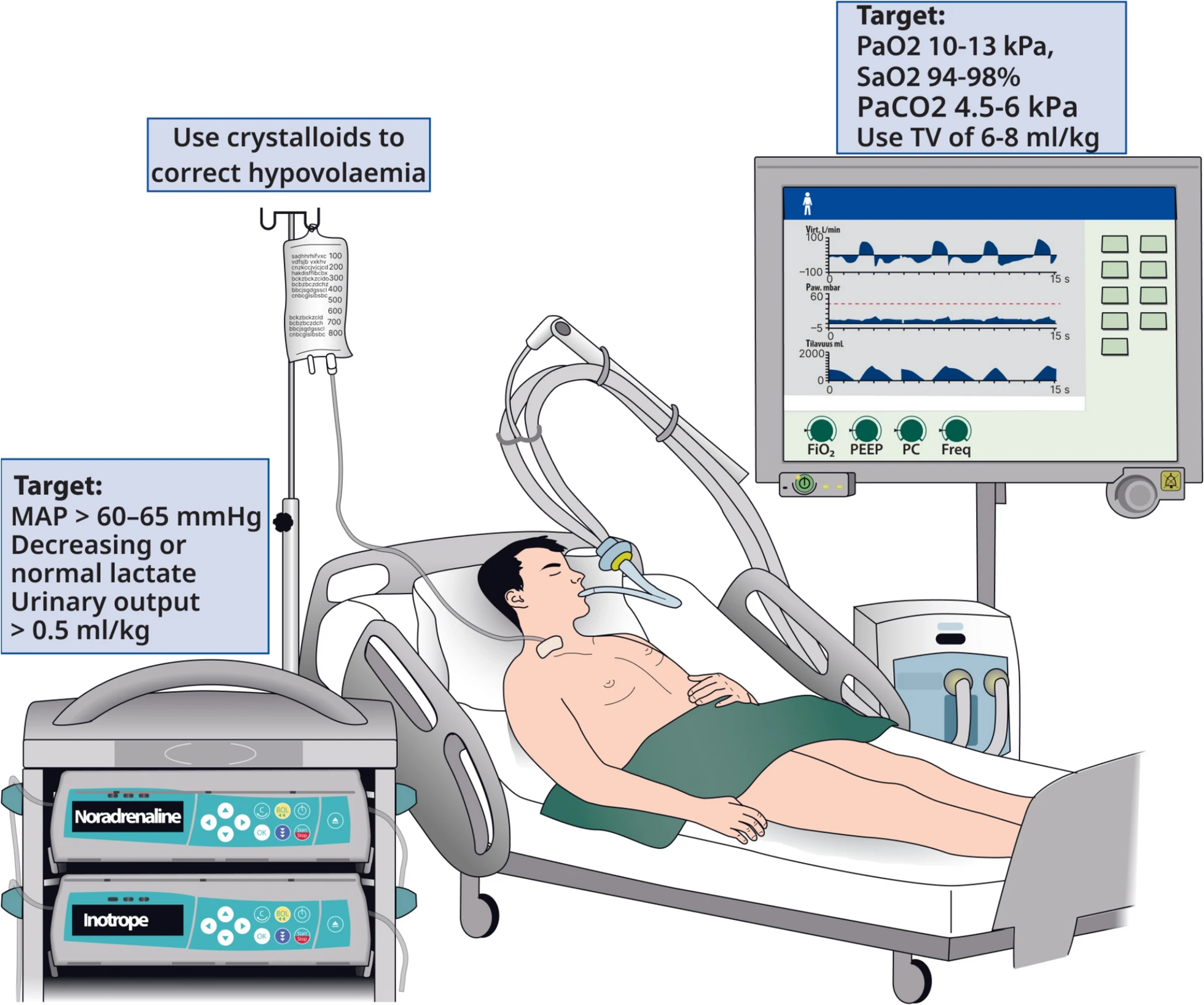
| Airway and Oxygenation Management | Recommendation to start with 100% oxygen immediately after ROSC, then titrate to 94–98% SpO₂ or PaO₂ 10–13 kPa (75–100 mmHg) | Maintains recommendation and adds explicit guidance highlighting inaccuracies in pulse oximetry in patients with darker skin tones |
| Ventilation Management | Recommended normocapnia (PaCO₂ 4.7–6.0 kPa (35–45 mmHg)) | Maintains recommendation with additional caution in patients with hypothermia, noting risk of hypocapnia |
| Coronary Reperfusion Strategy | Immediate coronary angiography strongly considered in OHCA without ST-elevation if high likelihood of coronary occlusion | Suggests delaying cardiac catheterisation if clinical context does not clearly indicate a high likelihood of acute coronary occlusion in OHCA patients without ST-elevation |
| Hemodynamic Management | Emphasised targeting MAP > 65 mmHg guided by adequate urine output and lactate normalization | Specifies MAP target of > 60–65 mmHg |
| Post-ROSC arrhythmias | Not included in any detail | Section added on recurrent and refractory arrhythmias post-ROSC |
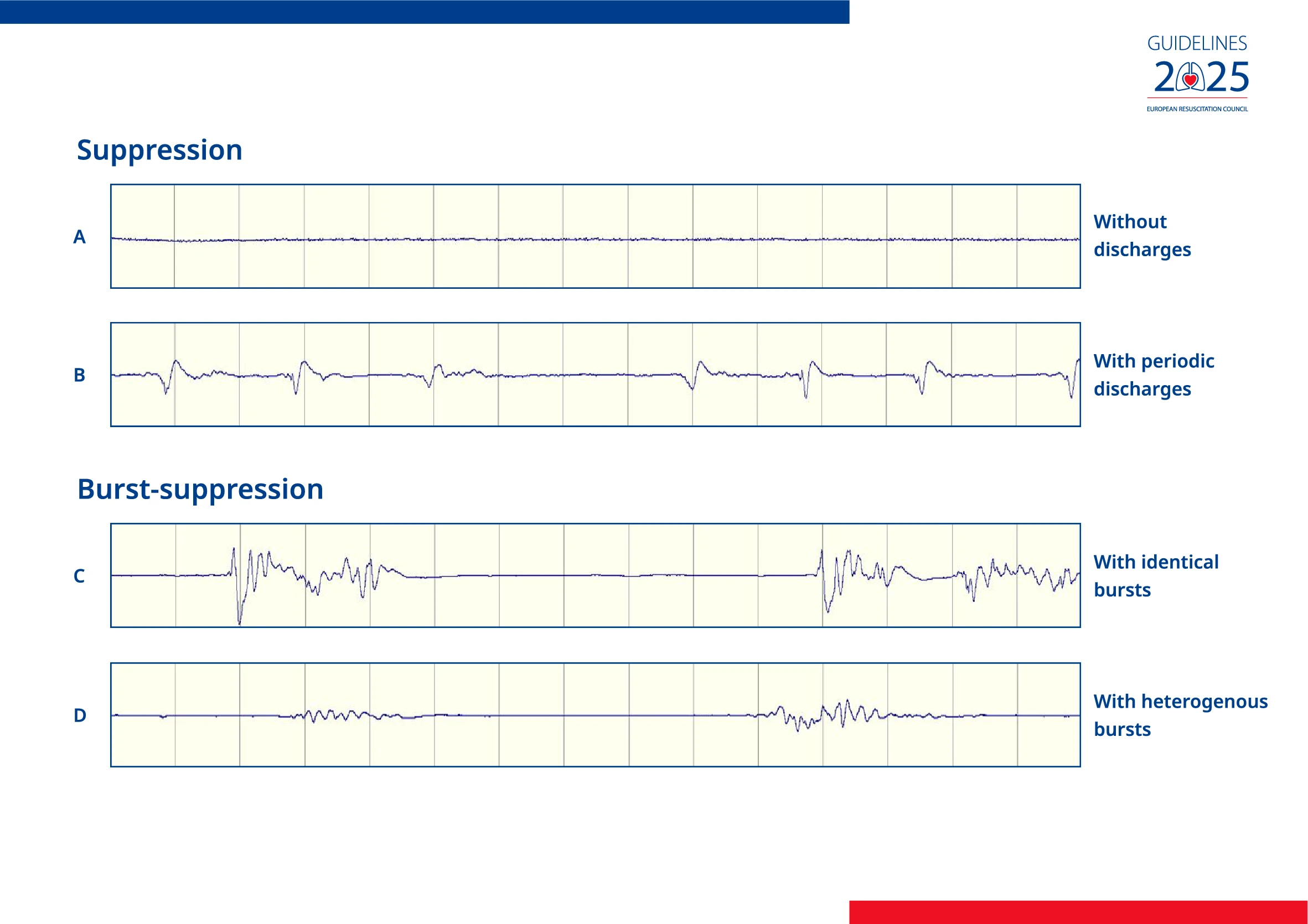
| Seizure Management | Recommended EEG monitoring | Explicitly states patients with myoclonus but benign EEG backgrounds should undergo wake-up trials days after arrest |
| Temperature Management | Recommended targeted temperature management at 32–36°C for at least 24 h and fever avoidance (> 37.7°C) for at least 72 h post-ROSC | Preferred terminology is temperature control. Recommends actively preventing fever by targeting a temperature of ≤ 37.5°C for at least 72 h post-ROSC |
| General Intensive Care Management | Recommended prophylactic stress ulcer prophylaxis and thromboembolism prophylaxis | Maintains previous recommendations. Emphasises using short-acting sedatives to facilitate neurological assessment, discourages routine neuromuscular blocking drugs unless severe acute respiratory distress syndrome |
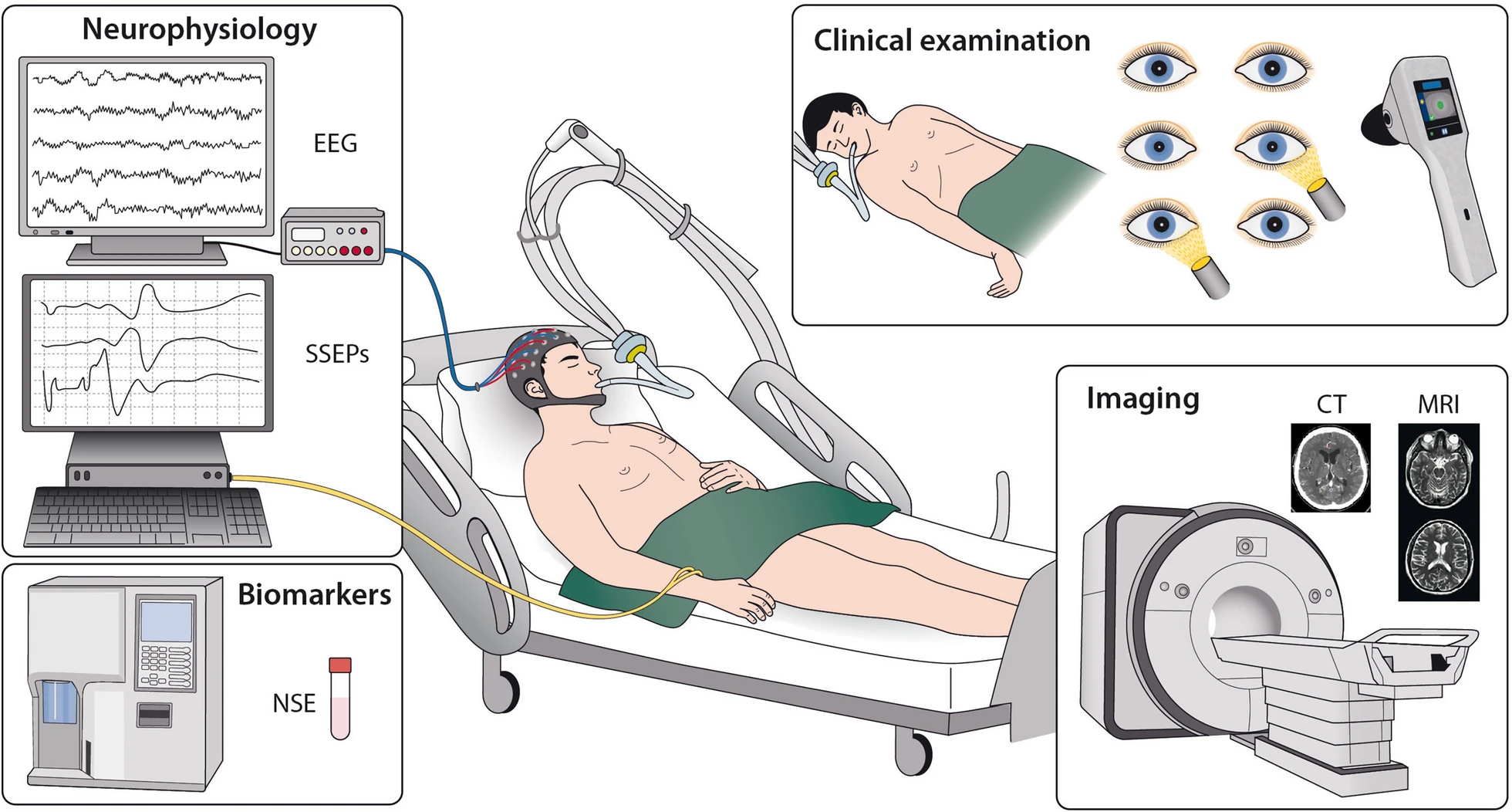
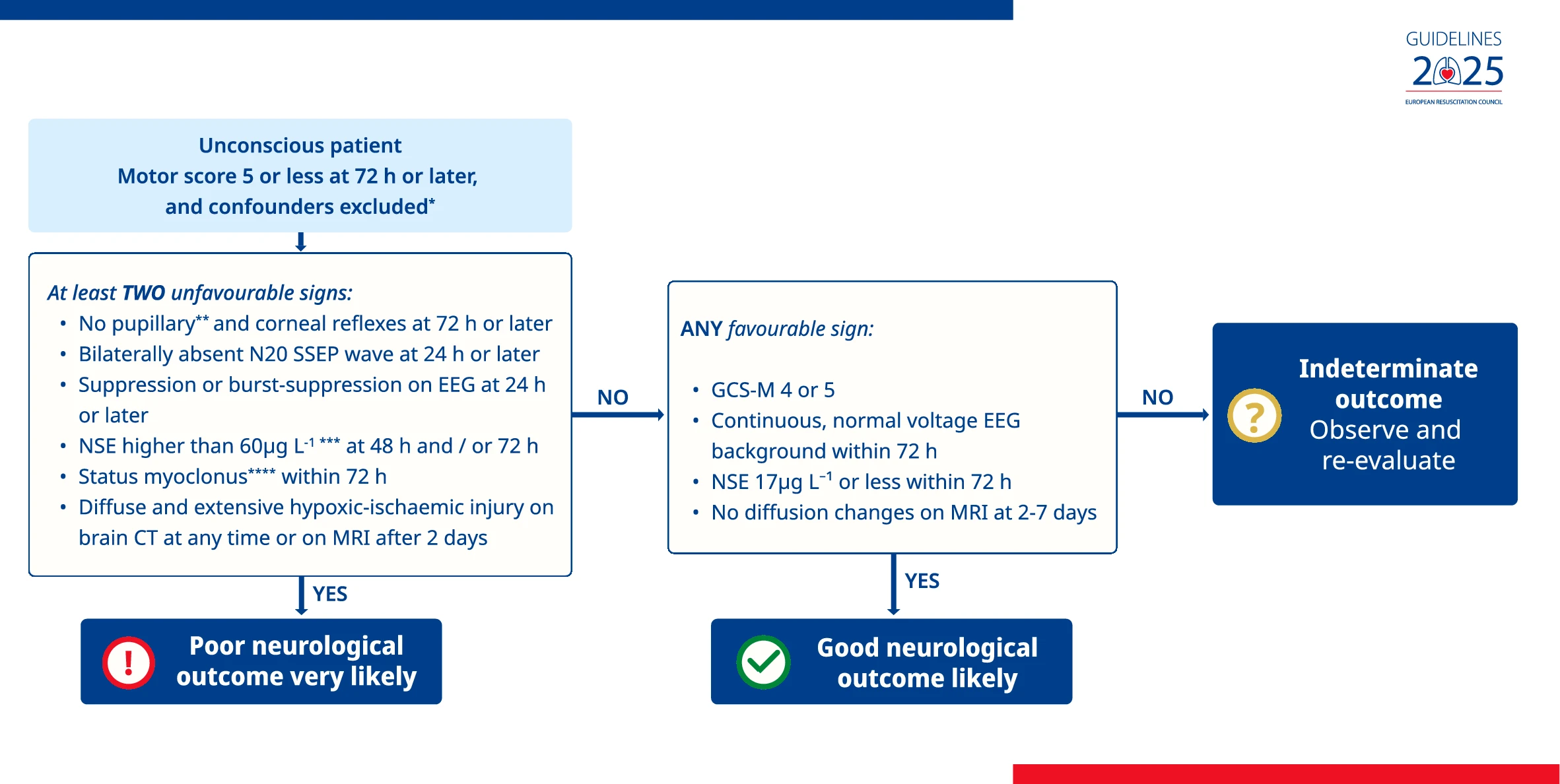
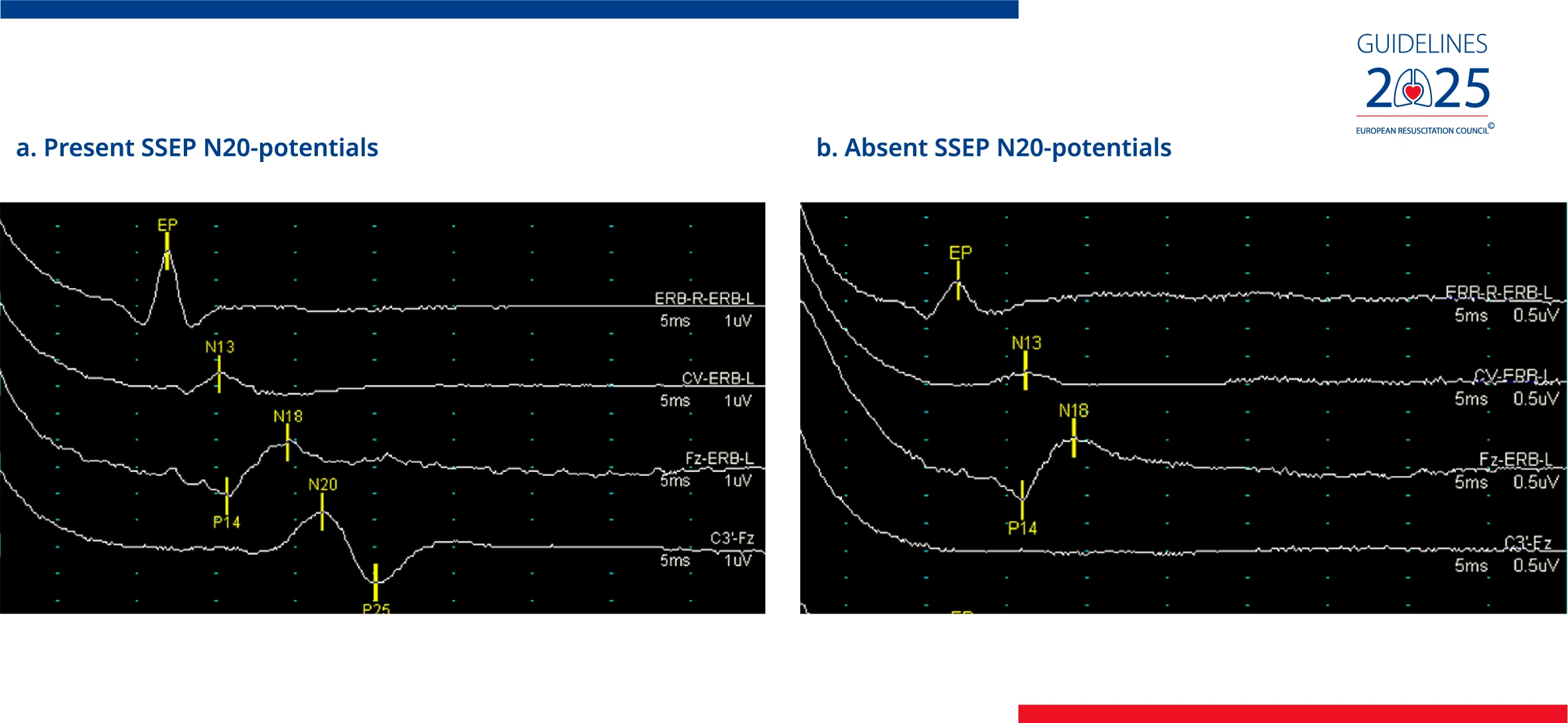
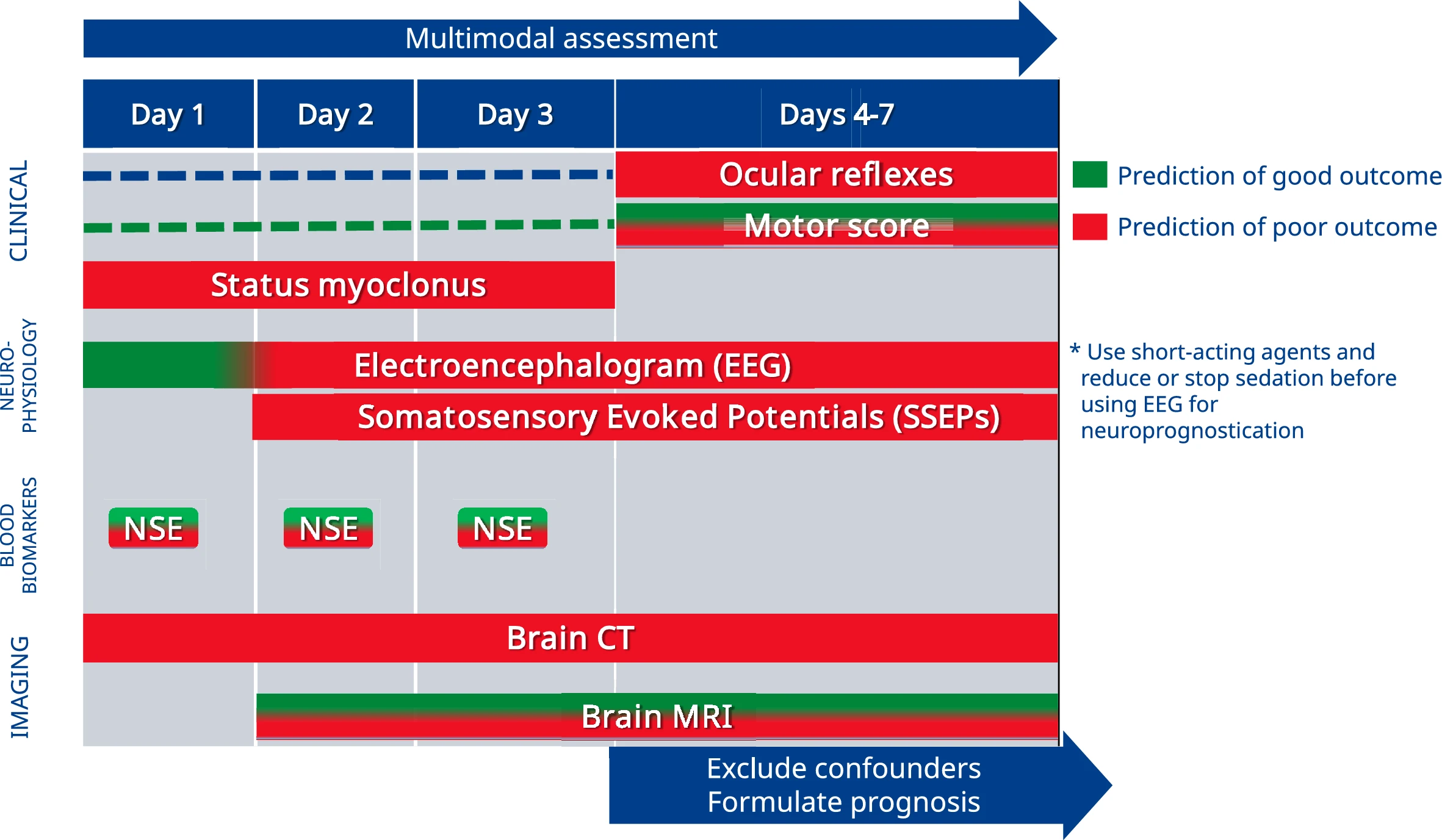
| Neurological Prognostication | Emphasised multimodal neurological assessment at ≥ 72 h | Extends the entry point of the algorithm to all unconscious patients (Glasgow Motor Score 5 or less). Maintains recommendation with specified indicators of favourable neurological outcome, and suggested timing for brain CT and SSEP recording |
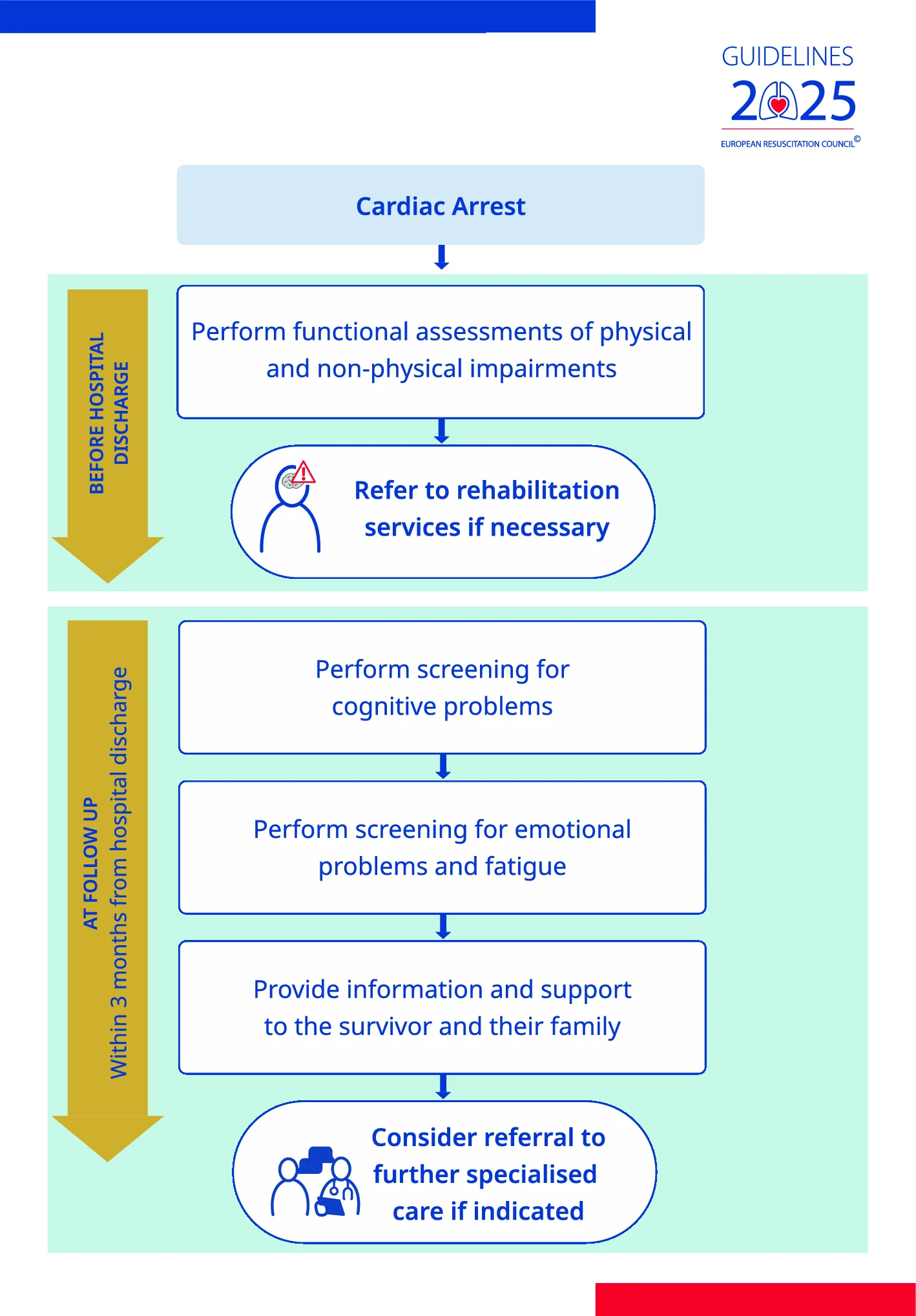
| Rehabilitation and Follow-up | Recommended functional assessment before discharge and follow-up within 3 months post discharge including screening of cognitive, emotional problems and fatigue. Brain injury and cardiac rehabilitation when indicated | Maintains recommendations and adds structured guidance on rehabilitation in the ICU including early mobilisation, delirium management, ICU diaries, and to address physical limitations during follow-up. Stronger focus on the involvement of co-survivors |
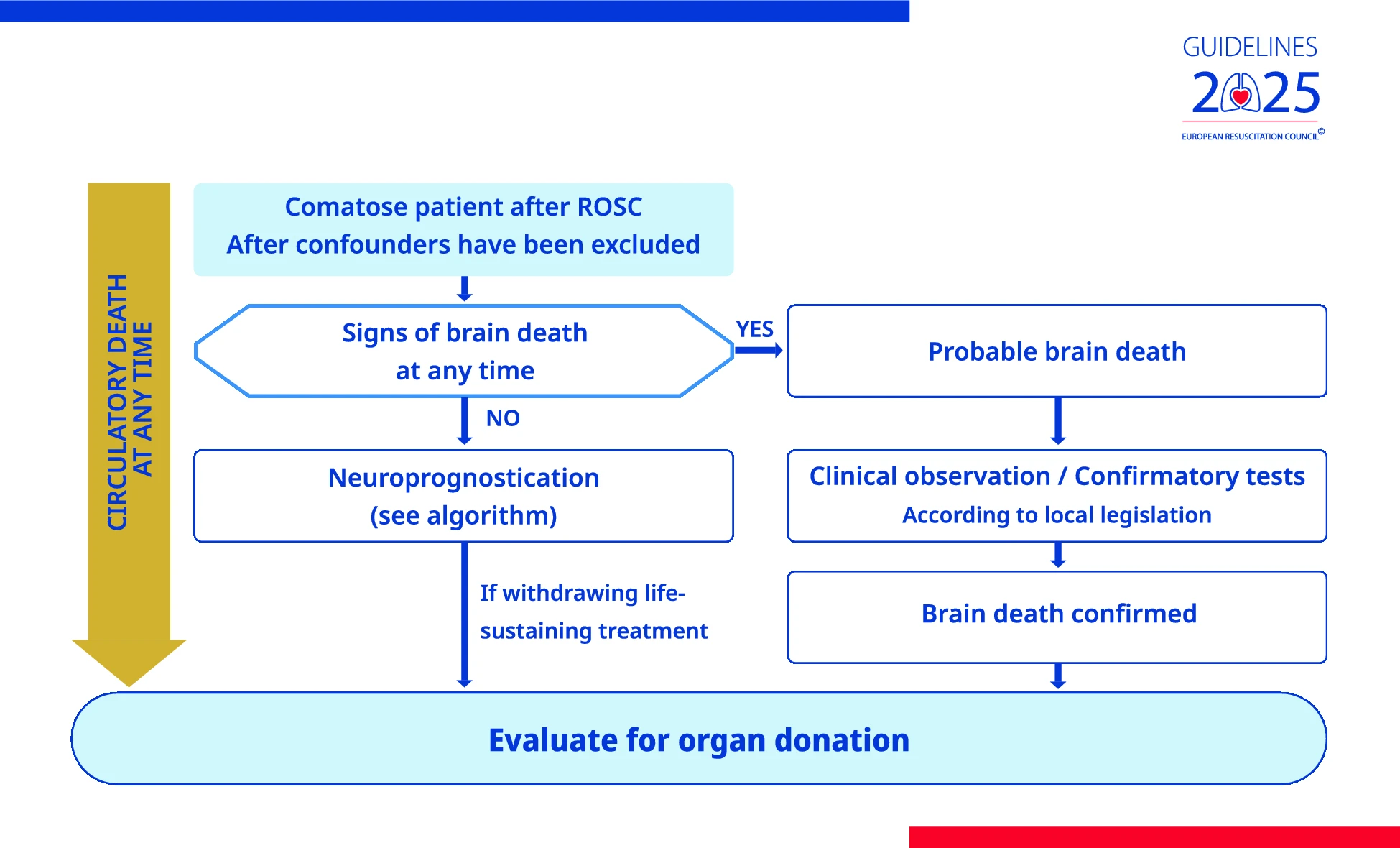
| Organ Donation | Recommended considering organ donation post-resuscitation | Maintains recommendation and adds recommendations for cardiac arrest registries to report organ donation activities |
| Investigating Unexplained Cardiac Arrest | Not included | New recommendations for comprehensive diagnostic work-up (including genetic testing, cardiac MRI, sodium channel blocker tests, exercise testing) and emphasises long-term follow-up |