Pulmonary Mucormycosis
Jonas Lötscher, Justus Baarts
N Engl J Med 2026;394:699
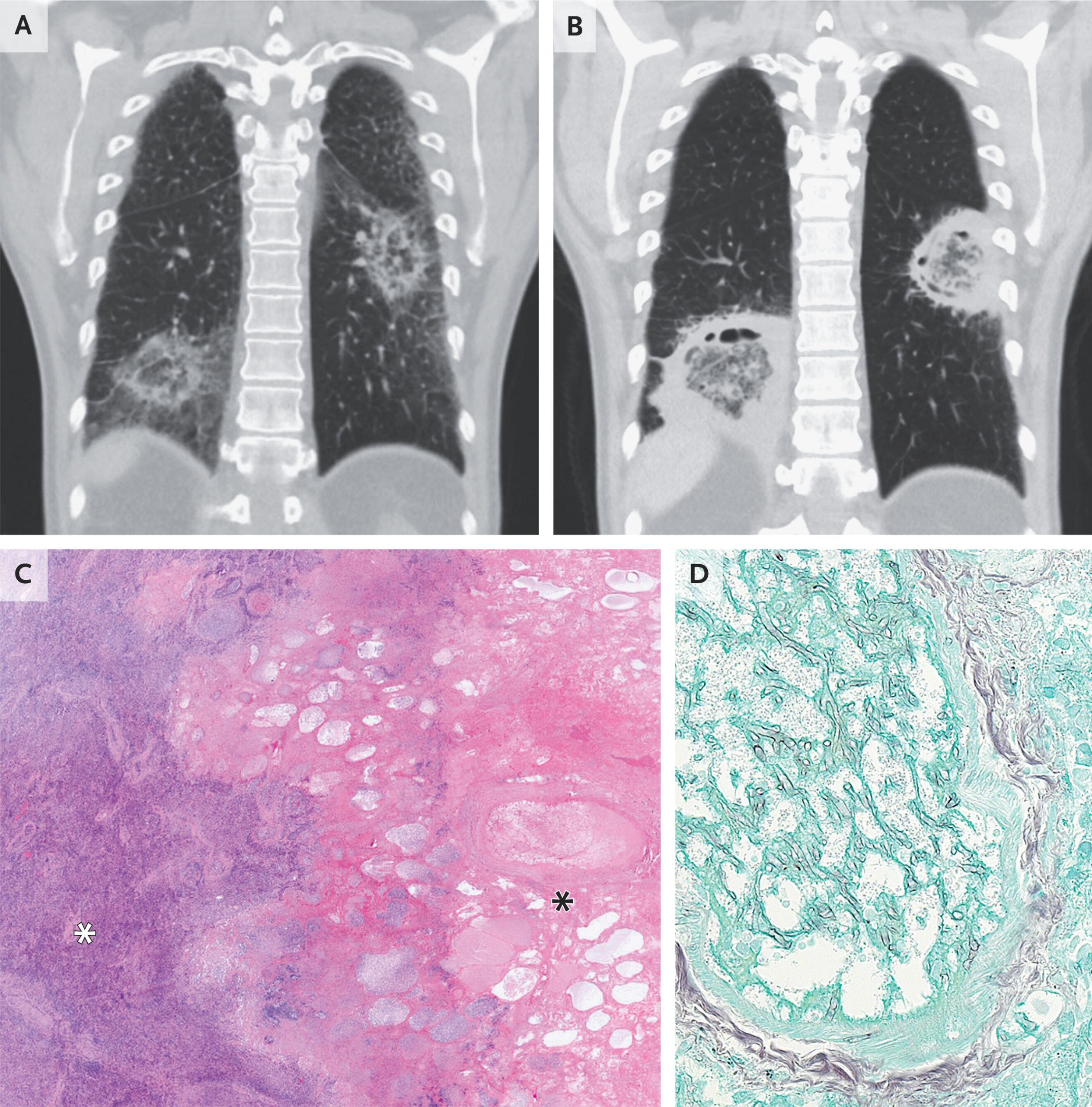
A 49-year-old man with acute myeloid leukemia who had been admitted to the hospital for induction chemotherapy was evaluated for prolonged neutropenic fever. On physical examination, crackles were heard at the lung bases. Computed tomography (CT) of the chest revealed rounded opacities with central ground-glass attenuation and ringlike peripheral consolidation in both lungs (Panel A, coronal view) — a finding known as the reversed halo sign that can occur with invasive fungal infections. Treatment with amphotericin B was started. A polymerase-chain-reaction (PCR) assay for mucorales species in bronchoalveolar lavage fluid was positive. After 2 weeks of treatment, repeat CT of the chest revealed increased attenuation of the ringlike peripheral consolidations and central cavitation of the opacities (Panel B, coronal view), findings consistent with neutrophil recovery. Surgical resection was performed. Histopathological analysis of the resected lung tissue showed central necrosis (Panel C, black asterisk; hematoxylin and eosin stain) surrounded by organizing pneumonia (Panel C, white asterisk). Intravascular hyphae were also seen (Panel D, Grocott’s methenamine silver stain). PCR analysis of the resected tissue identified Rhizomucor pusillus, which confirmed the diagnosis of pulmonary mucormycosis. One week after surgery, the patient was discharged home with a prescription for isavuconazole for secondary prophylaxis. Two weeks later, he underwent allogeneic hematopoietic stem-cell transplantation