Airway Management in Patients With Acute Traumatic Brain Injury: An Evidence-Based Approach
- In ICU
- Thu, 24 Jul 2025
ICU Management & Practice, Volume 25 - Issue 3, 2025
This review highlights airway management in traumatic brain injury, focusing on strategies to prevent secondary brain injury. Key interventions include advanced preoxygenation, haemodynamic stabilisation, cautious sedation, selective use of prehospital intubation or supraglottic devices, protective ventilation, and early antibiotic prophylaxis to reduce ventilator-associated pneumonia.
Introduction
Traumatic brain injury (TBI) remains a major cause of morbidity and mortality worldwide, with airway compromise representing a critical concern in its acute management. Hypoxaemia, hypercapnia, and haemodynamic instability are recognised contributors to secondary brain injury and are frequently encountered during emergency airway interventions. Consequently, early and appropriate airway management in patients with TBI is essential to minimise further neurological deterioration. While the Brain Trauma Foundation (BTF) and other expert guidelines offer general recommendations for airway protection, several key controversies persist. These include the optimal timing and location for intubation (prehospital vs. in-hospital), the choice of preoxygenation strategy, haemodynamic optimisation, the use of neuromuscular blocking agents, and appropriate ventilator settings. Furthermore, recent evidence has prompted a re-evaluation of prehospital intubation practices and highlighted the role of supraglottic airway devices as safe alternatives when endotracheal intubation is not feasible.
This review synthesises current evidence and expert recommendations for airway management in adult TBI patients, emphasising strategies that mitigate secondary brain injury. It highlights key interventions, such as preoxygenation techniques, haemodynamic optimisation, and ventilatory strategies, based on recent clinical trials and updated guidelines.
From a physiological perspective, TBI represents a sudden and severe disruption of cerebral homeostasis. Based on the biomechanical characteristics involved in the injury mechanism, TBI is typically classified into three main types. The first is closed TBI, characterised by an impact that does not compromise the integrity of the skull, resulting in internal brain injuries caused by acceleration-deceleration forces and the displacement of brain tissue. The second type is penetrating TBI, in which an external object breaches the skull and causes direct damage to the brain parenchyma. The third type is blast-induced TBI, usually associated with explosions, where energy is transmitted through pressure waves, leading to neurological dysfunction without direct physical contact with the skull (Ng and Lee 2019; Dixon 2017).
The clinical severity of these injuries varies widely and is associated with different levels of morbidity, commonly assessed using the Glasgow Coma Scale (GCS), a standardised tool for evaluating consciousness and guiding early prognosis (Teasdale et al. 2014). Clinical outcomes are determined by the dynamic interplay between primary and secondary injury processes. Primary injury occurs at the moment of impact and involves immediate structural damage to the brain parenchyma, such as cortical contusions, intraparenchymal or subdural haemorrhages, and diffuse axonal injuries resulting from acceleration-deceleration forces. In contrast, secondary injury develops progressively and is mediated by a complex cascade of biochemical, cellular, and haemodynamic events, including glutamatergic excitotoxicity, mitochondrial dysfunction, oxidative stress, and disruptions in cerebral autoregulation. These processes contribute to delayed neurological deterioration and expansion of the initial brain injury (Thapa et al. 2021). , critical mechanisms of secondary injury are hypoxia, cerebral ischaemia, excitotoxicity, mitochondrial failure, and, notably, intracranial hypertension (ICH), a major complication in TBI patients due to its detrimental effects on cerebral perfusion. According to the Monro-Kellie doctrine, intracranial volume is fixed and consists of brain tissue, blood, and cerebrospinal fluid (CSF) (Cucciolini et al. 2023). An increase in any of these components, in the absence of effective compensatory mechanisms, leads to elevated intracranial pressure (ICP). When ICP exceeds cerebral perfusion pressure (CPP), cerebral blood flow (CBF) is reduced, potentially resulting in ischaemia and cerebral infarction.
Patient Preparation and Optimisation in Traumatic Brain Injury
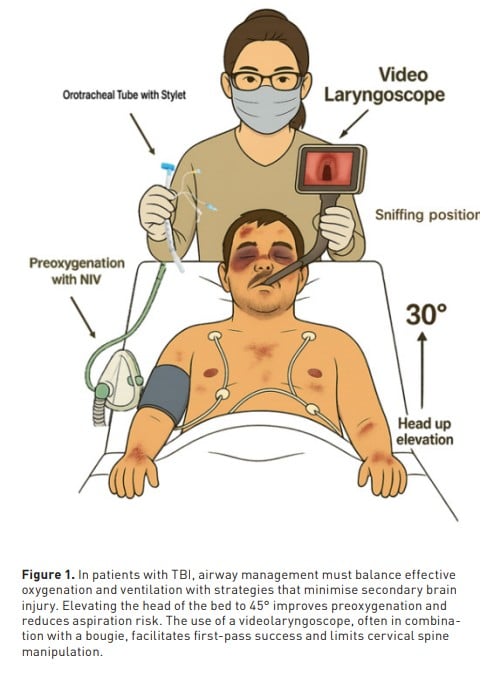
In patients with TBI, particularly those with intracranial hypertension, the airway is, by definition, physiologically difficult (Karamchandani et al. 2024). Careful preparation prior to tracheal intubation is, therefore, essential to minimise the risk of secondary brain injury and cardiovascular collapse (Figure 1). According to the recommendations of the Society of Critical Care Anesthesiologists (SOCCA), pre-intubation airway assessment should be performed whenever feasible to identify anatomical and technical challenges. Haemodynamic optimisation with vasopressors and/or inotropes should be pursued proactively. Preoxygenation using non-invasive ventilation with pressure support and positive end-expiratory pressure (PEEP) is the preferred method to reduce oxygen desaturation and can be supplemented with apnoeic oxygenation via high-flow nasal cannula. Gentle mask ventilation during the apnoeic phase of rapid sequence intubation may be used when necessary to maintain adequate oxygenation. Laryngoscopy and intubation with the patient in the sniffing position may increase the incidence of successful intubation on the first attempt (DeMasi et al. 2025). The Head-Elevated Laryngoscopic Position (HELP), with the head of the bed elevated to 45 degrees, is recommended to enhance glottic visualisation and reduce aspiration risk. Point-of-care ultrasound, when available, may further support clinical decision-making by facilitating the assessment of cardio-respiratory status.
Importantly, achieving a successful and swift first intubation attempt is associated with better outcomes in critically ill patients. In this context, video laryngoscopy should be considered the first-line technique. A secondary analysis of the DEVICE trial (Muhs et al. 2025) demonstrated that, among patients intubated after cardiac arrest, video laryngoscopy significantly increased first-attempt success rates (83.3% vs. 64.6%) and shortened the duration of laryngoscopy compared to direct laryngoscopy. Additionally, a recent network meta-analysis (de Carvalho et al. 2025) comparing various laryngoscopic devices in over 44,284 patients found that channelled and hyperangulated videolaryngoscopes were associated with the lowest rates of failed first attempts, better glottic views, and fewer complications, including oesophageal intubation and airway trauma. These benefits were not observed with video stylets alone, highlighting the importance of selecting a videolaryngoscope design that facilitates both visualisation and tube delivery, particularly in patients with physiologically difficult airways, such as those with TBI and intracranial hypertension. Additionally, to increase the first-attempt success rate during intubation, adjuncts such as a bougie or stylet may be used. A systematic review and meta-analysis assessing the association between bougie use and first-attempt intubation success found that bougie use was associated with a higher success rate (RR 1.11, 95% CI 1.06–1.17), particularly in patients with difficult airways classified as Cormack-Lehane grade III or IV (RR 1.60, 95% CI 1.40–1.84) (von Hellmann et al. 2024).
Effects of Medications During Induction on Haemodynamic Stability and Intracranial Pressure
During rapid sequence intubation, it is essential to implement neuroprotective strategies that guide the selection of the most appropriate sedative agent, prioritising those with minimal adverse effects on haemodynamic stability. Arterial hypotension, regardless of its duration, is strongly associated with increased mortality in patients with TBI, as highlighted by Godoy et al. (2021). Therefore, maintaining an adequate CPP is a critical objective to minimise the risk of secondary brain injury.
Ketamine is an anaesthetic agent known for its haemodynamic stability, as it does not reduce blood pressure, making it a preferred choice in many critically ill patients (Hu et al. 2024). Historically, concerns have been raised about its potential to increase ICP. However, contrary to this assumption, a randomised controlled (Bar-Joseph et al. 2009) evaluated children with refractory intracranial hypertension (ICP >18 mmHg) who had failed first-tier ICP management. Following administration of ketamine at a dose of 1–1.5 mg/kg, ICP significantly decreased by 30% (from 25.8 ± 8.4 to 18.0 ± 8.5 mmHg; p < 0.001), while CPP increased from 54.4 ± 11.7 to 58.3 ± 13.4 mmHg (p < 0.005). These findings demonstrate that ketamine not only fails to increase ICP but also effectively reduces it, preventing further elevations during potentially distressing procedures without inducing hypotension or compromising CPP. These results are further supported by a systematic review and meta-analysis (Zeiler et al. 2014), which concluded that ketamine is safe for patients with severe TBI and may, in fact, contribute to lowering ICP in this context.
Propofol is one of the most commonly used hypnotic agents; however, its haemodynamic effects may impact cerebral perfusion pressure (Kotani et al. 2023). A systematic review and meta-analysis demonstrated that propofol significantly reduces intracranial pressure (mean difference: −4.06 mmHg; p < 0.00001) and is associated with a lower risk of nausea and vomiting (risk ratio = 0.59; p= 0.002) (Liu et al. 2024). A study comparing the effectiveness of ketamine versus propofol during rapid sequence induction in trauma patients found no significant difference in 30-day mortality between the two groups (20.2% for ketamine vs. 22.8% for propofol; p= 0.46). Additionally, there was no significant association between the choice of induction agent and hospital length of stay, ICU stay, or duration of mechanical ventilation (Breindahl et al. 2021). Therefore, in settings where both ketamine and propofol are available, either agent may be considered safe and appropriate for use, depending on the clinical context and patient-specific factors. In the management of TBI, opioids are frequently employed to control pain and ensure patient comfort—goals commonly recommended in the literature (Taccone et al. 2020). Fentanyl, in particular, administered at doses of 2–3 µg/kg, acts as a sympatholytic agent that helps attenuate increases in blood pressure and intracranial pressure during laryngoscopy (Hoyne et al. 2025). However, the effects of opioids on cerebral haemodynamics have been questioned, especially in the setting of TBI. A systematic review evaluated the impact of opioids before and after administration, compared various opioids, and analysed the effects of opioids versus other sedatives. The review found—with level 1 evidence—that bolus administration of morphine, fentanyl, and sufentanil increases ICP and decreases CPP and mean arterial pressure (MAP). Conversely, when administered as continuous infusions, these opioids do not appear to affect cerebral haemodynamics or ICP. It is important to note that the haemodynamic effects associated with bolus administration are transient. Therefore, the use of opioids, including fentanyl, can be considered safe in patients with TBI, particularly when administered carefully and titrated based on the clinical scenario (Wiener et al. 2019).
A key objective during tracheal intubation is to minimise the risk of failure and avoid airway trauma. The use of neuromuscular blocking agents (NMBAs) has been shown to improve intubating conditions and reduce complications associated with difficult airway management (Lundstrom et al. 2017; Wilcox et al. 2012). Rocuronium is commonly employed at a dose of 1.2 mg/kg, corresponding to approximately 4 times the ED₉₅—the effective dose that suppresses 95% of baseline twitch response (Renew et al. 2020). Beyond facilitating intubation, neuromuscular blockade may also aid in controlling ICP. Among available agents, non-depolarising NMBAs are preferred over succinylcholine, given their more favourable profile with respect to transient ICP elevation (Sanfilippo et al. 2015).
Impact of O₂ and CO₂ in Patients With TBI
In the context of TBI, optimal management of oxygenation and ventilation is vital, as disturbances in oxygen (O₂) and carbon dioxide (CO₂) levels can significantly exacerbate secondary brain injury. One key pathophysiological mechanism is oxidative imbalance, which may result from sustained hyperoxaemia. This condition promotes excessive production of reactive oxygen species (ROS), overwhelming the body’s antioxidant defences and triggering lipid peroxidation. This process disrupts the integrity of cellular membranes, exacerbates neuronal damage, and contributes to the progression of secondary brain injury (Ottolenghi et al. 2020). Moreover, inadequate ventilation leading to persistent abnormalities in oxygenation of arterial carbon dioxide tension (PaCO₂) may have deleterious consequences. Hypoxaemia is directly associated with increased cerebral ischaemia, whereas hyperoxaemia, although traditionally considered beneficial, may induce neuronal apoptosis and necrosis under conditions of excessive oxidative stress (Godoy et al. 2023; Taccone et al. 2020).
With regard to CO₂, hypocapnia induced by hyperventilation can provoke cerebral vasoconstriction, reducing cerebral blood flow and worsening ischaemia. Conversely, moderate hypercapnia may induce vasodilation of cerebral arteries, potentially contributing to or exacerbating cerebral oedema in certain scenarios (Soto-Páramo et al. 2022). From a physiological standpoint, adequate oxygen delivery (DO₂) to brain tissue depends on two fundamental components: sufficient cerebral blood flow (CBF) and adequate arterial oxygen content (CaO₂). The latter is determined by factors such as arterial oxygen saturation, haemoglobin concentration, and partial pressure of arterial oxygen (PaO₂). Disruption of either component compromises oxygen delivery to neuronal tissue, increasing the risk of tissue hypoxia, cerebral ischaemia, and progressive secondary injury (Hoiland et al. 2019).
Criteria for Intubation in Acute Brain Injury
Since its introduction into clinical practice in 1974, the Glasgow Coma Scale (GCS) has traditionally served as the principal criterion for determining the need for intubation in patients with TBI. A GCS score below 8 has classically indicated the need for airway protection, based on the assumption that such patients are unable to maintain protective airway reflexes. However, this relationship is not absolute. In a prospective observational study involving 208 patients, Rotheray et al. (2012) assessed the correlation between GCS and airway protective reflexes. They found that 22.1% of patients with a GCS > 15 lacked a gag reflex, and 25.7% lacked a cough reflex. Conversely, among patients with GCS < 8, 36.4% preserved a normal gag reflex, and 24.2% retained a cough reflex. These findings suggest that although a lower GCS score is associated with a higher probability of impaired airway reflexes, a substantial proportion of patients with low scores still retain airway protection capabilities. Despite these limitations, the GCS remains the most widely used tool for assessing coma and guiding decisions regarding airway management. Nonetheless, some investigators have highlighted its shortcomings, particularly in patients with evolving neurological deterioration. To address these limitations, the Full Outline of UnResponsiveness (FOUR) score was developed. This scale evaluates four components: eye response, motor response, brainstem reflexes, and respiration.
Okasha et al. (2014)compared the predictive performance of the GCS and the FOUR score for endotracheal intubation in TBI patients. They reported a higher area under the curve (AUC) for the FOUR score (0.982 vs. 0.96 for GCS), although the difference was not statistically significant (p = 0.06). A FOUR score cutoff of <11 demonstrated 79% sensitivity and 100% specificity, while a GCS cutoff of <8 showed 87% sensitivity and 100% specificity. These results support the use of a FOUR score <11 as an additional indicator for airway intervention in patients with TBI. While a GCS <8 remains a pragmatic threshold for airway protection, integrating assessments of airway reflexes or using the FOUR score may refine decision-making, especially in equivocal cases.
Prehospital vs In-Hospital Intubation
Emergency medical services (EMS) are often the first responders at the scene and play a pivotal role in the initial assessment and stabilisation of patients with TBI. While guidelines, such as those established by the Brain Trauma Foundation (BTF), provide clear recommendations for airway management, they also acknowledge that, when personnel are adequately trained, prehospital intubation may be warranted, particularly in the presence of hypoxaemia (Hawryluk et al. 2023). However, recent evidence has questioned the mortality benefit of this approach. A 2024 systematic review and meta-analysis evaluated the impact of prehospital airway management on mortality in patients with severe TBI. The pooled odds ratio (OR) for mortality associated with prehospital intubation was 0.89 [95% confidence interval (CI) 0.65–1.23; p = 0.48; I² = 96%], suggesting no statistically significant benefit. A subgroup analysis of randomised controlled trials (RCTs) yielded an OR of 0.67 (95% CI 0.23–1.94; p = 0.46; I² = 57.35%), further reinforcing the absence of a mortality advantage linked to prehospital airway intervention (Shafique et al. 2024).
Supraglottic airway (SGA) devices have emerged as valuable tools in the emergency management of trauma patients, particularly in situations where orotracheal intubation may be technically challenging. These devices offer advantages such as reduced technical complexity and the possibility of placement without the need for sedative or paralytic agents. According to the 2023 BTF guidelines, trained EMS personnel may consider the use of SGAs in the prehospital setting (Hawryluk et al. 2023). A potential concern with both endotracheal intubation and SGA placement is the transient elevation of ICP caused by sympathetic stimulation during airway manipulation. To assess this, a prospective study evaluated the haemodynamic impact and optic nerve sheath diameter (ONSD)—a surrogate marker for ICP—following placement of three different SGA devices: i-gel, ProSeal Laryngeal Mask Airway (LMA), and Supreme LMA. The study found no statistically significant differences in ONSD across the three groups, with average values ranging from 4.8 to 5.9 mm (p > 0.05), suggesting that these devices do not substantially influence ICP and may be considered safe alternatives for airway management in patients with TBI (Okyay et al. 2023).
In the context of RSI, meticulous attention must be paid to avoid procedure-related complications that could worsen primary brain injury or precipitate secondary brain insults. Core strategies focus on the prevention of hypoxaemia, hypo/hypertension, hypo/hypercapnia, and the sympathetic surge induced by laryngoscopy. In addition, clinicians must be vigilant to avoid difficult airway scenarios and mitigate abrupt changes in intrapulmonary pressures resulting from the initiation of positive pressure ventilation or the application of positive end-expiratory pressure (PEEP) (Hoyne et al. 2025).
Avoiding Hypoxaemia
Hypoxaemia remains a central concern during airway management in patients with acute brain injury, as it is a well-established contributor to secondary neuronal damage (Rajajee et al. 2017). Modern approaches to mitigate this risk emphasise the use of non-invasive positive pressure ventilation (NIPPV) during preoxygenation. In critically ill patients undergoing endotracheal intubation, a preoxygenation strategy using BiPAP, delivered for a minimum of 3 minutes with FiO₂ 100%, EPAP >5 cmH₂O, IPAP >10 cmH₂O, and a respiratory rate >10 breaths/min, has demonstrated a clear clinical advantage. In a comparative study, the incidence of hypoxaemia was 9.1% in the NIPPV group (57/624) versus 18.5% in the oxygen mask group (118/637), yielding an absolute risk reduction of 9.4 percentage points (95% CI −13.2 to −5.6; p < 0.001) and a low aspiration rate of only 0.9%, supporting NIPPV as a safe and effective option (Gibbs et al. 2024). These findings are corroborated by a systematic review and meta-analysis, which demonstrated that positive pressure ventilation significantly reduces hypoxaemia compared to standard facemask oxygenation (RR 0.51 [0.39–0.65]; p < 0.001; high certainty). Additionally, high-flow nasal cannula (HFNC) was also superior to facemask oxygen (RR 0.69 [0.54–0.88]; p = 0.0064; high certainty). Collectively, this evidence supports the use of NIPPV and HFNC as effective preoxygenation strategies to minimise hypoxaemia during intubation in neurologically vulnerable patients (Pitre et al. 2025; Robba et al. 2024).
Blood Pressure Optimisation
Haemodynamic instability is a frequent complication during airway management, occurring in up to 42.6% of critically ill patients undergoing intubation (Russotto et al. 2021). To ensure adequate cerebral perfusion, current guidelines recommend maintaining a mean arterial pressure (MAP) of 80–100 mmHg. Alternatively, systolic blood pressure (SBP) targets are stratified by age: >100 mmHg for patients aged 50–69 years, and >110 mmHg for those aged 18–49 or ≥70 years. Although some authors advocate for pre-intubation intravenous fluid administration as a preventive strategy, a randomised controlled trial found no significant difference in the incidence of cardiovascular collapse between patients who received a fluid bolus and those who did not (21.0% vs. 18.2%; absolute difference 2.8%; 95% CI −2.2 to 7.7; p = 0.25) (Russell et al. 2022). Consequently, in hypotensive patients, vasopressor therapy is the preferred approach to optimise blood pressure prior to or during intubation.
Ventilation Strategies
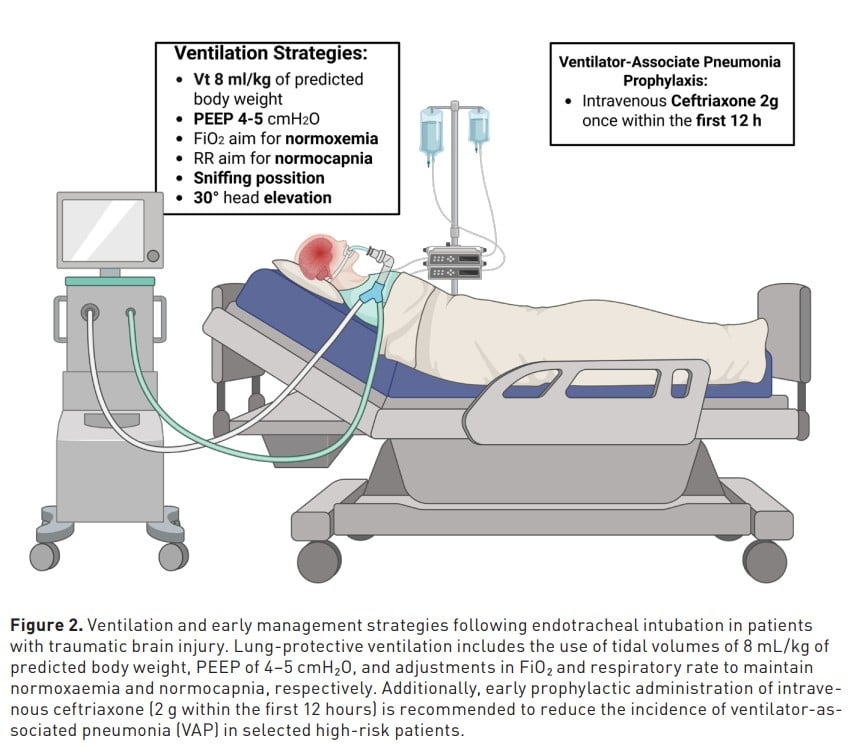
The cornerstone of mechanical ventilation in patients with brain injury is the maintenance of normocapnia. Both hypocapnia and hypercapnia have been independently associated with increased in-hospital mortality (p = 0.0009) (Russotto et al. 2021). Clinical guidelines recommend maintaining arterial CO₂ levels (PaCO₂) between 35–45 mmHg (Hoyne et al. 2025). In cases of severe TBI with elevated intracranial pressure (ICP), deep sedation is recommended to reduce metabolic demand and mitigate ICP spikes. The PROLABI trial assessed a lung-protective ventilation strategy in brain-injured patients without ARDS. Although it found no significant benefit regarding a composite outcome of mortality, ventilator liberation, or ARDS incidence, neurological outcomes at day 28 were worse in the protective ventilation group (61.5% vs. 45.3%; RR 1.35; 95% CI 1.03–1.79; p = 0.025) (Mascia et al. 2024). Conversely, the VENTIBRAIN study, a large observational analysis, described contemporary ventilation practices in patients with acute brain injury. A protective strategy—tidal volume (VT) of 6.5 mL/kg predicted body weight (IQR: 4.7–7.3), PEEP 5 cmH₂O (IQR: 5–8), and plateau pressure (Pplat) 15 cmH₂O (IQR: 13–18)—was associated with reduced mortality. Importantly, increasing plateau pressure was independently associated with mortality (HR 1.50; 95% CI 1.27–1.78) (Robba et al. 2025). Based on these findings, optimal ventilation strategy in patients with acute brain injury includes (Figure 2):
- VT 8 mL/kg of predicted body weight
- Pplat <15 cmH₂O
- and avoidance of excessive PEEP and FiO₂
Prevention of Early Ventilator-Associated Pneumonia
Ventilator-associated pneumonia (VAP) is a common complication in patients with TBI who require mechanical ventilation. Recent evidence supports the use of early antibiotic prophylaxis to reduce the incidence of this complication. A multicentre, randomised, double-blind, placebo-controlled trial evaluated the effect of a single dose of intravenous ceftriaxone (2 g) administered within 12 hours after intubation in patients expected to require mechanical ventilation for at least 48 hours. The study demonstrated a significant reduction in the incidence of early VAP in the ceftriaxone group compared to placebo (14% vs. 32%; hazard ratio 0.60 [95% CI 0.38–0.95]; p = 0.030), without adverse effects attributable to the intervention or evidence of microbiological resistance (Dahyot-Fizelier et al. 2024). This finding supports early targeted prophylaxis as an effective and safe strategy to prevent early-onset VAP in the context of acute brain injury.
Controversies and New Approaches
Despite advancements in airway management, several controversies persist in the care of patients with TBI. One of the most debated topics is the role of prehospital intubation. While theoretically beneficial in preventing hypoxaemia, current evidence does not demonstrate a clear mortality benefit and raises concerns about potential harm in the absence of optimal provider training and conditions. The use of supraglottic airway devices has emerged as a viable alternative in prehospital and emergency settings, particularly when rapid intubation is not feasible. Additionally, growing emphasis has been placed on optimising preoxygenation strategies to prevent hypoxaemia during intubation, with non-invasive ventilation and high-flow nasal cannula outperforming conventional facemask oxygen. In haemodynamic management, while fluid boluses have limited impact, early vasopressor use appears to be more effective in maintaining cerebral perfusion. Recent studies have also refined our understanding of protective ventilation, suggesting that overly aggressive lung-protective strategies may worsen neurological outcomes, whereas moderate PEEP and low plateau pressures provide a more balanced approach. Lastly, early prophylaxis against ventilator-associated pneumonia, such as with a single dose of ceftriaxone, has shown promise in reducing infection rates without increasing antimicrobial resistance, representing a novel adjunct to early TBI management.
Conclusion
Airway management in patients with TBI requires a delicate balance between timely intervention and the prevention of secondary brain injury. Current evidence supports the use of advanced preoxygenation techniques, early haemodynamic stabilisation with vasopressors, assess the risks and benefits of prehospital intubation and consider supraglottic airway devices, moderate protective ventilation strategies and early antibiotic prophylaxis for ventilator-associated pneumonia to optimise outcomes.
Conflict of Interest
None.
References:
Bar-Joseph G, Guilburd Y, Tamir A, Guilburd JN. Effectiveness of ketamine in decreasing intracranial pressure in children with intracranial hypertension. J Neurosurg Pediatr. 2009;4(1):40-46.
Breindahl N, Baekgaard J, Christensen RE, et al. Ketamine versus propofol for rapid sequence induction in trauma patients: a retrospective study. Scand J Trauma Resusc Emerg Med. 2021;29:136.
Cucciolini G, Motroni V, Czosnyka M. Intracranial pressure for clinicians: it is not just a number. J Anesth Analg Crit Care. 2023;3(1):31.
Dahyot-Fizelier C, Lasocki S, Kerforne T, et al. Ceftriaxone to prevent early ventilator-associated pneumonia in patients with acute brain injury: a multicentre, randomised, double-blind, placebo-controlled, assessor-masked superiority trial. Lancet Respir Med. 2024;12(5):375-385.
de Carvalho CC, Guedes IHL, Dantas MVM, et al. Videolaryngoscope designs for tracheal intubation in adults: a systematic review with network meta-analysis of randomised controlled trials. Anaesthesia. 2025 Mar 11.
DeMasi SC, Casey JD, Semler MW. Evidence-based emergency tracheal intubation. Am J Respir Crit Care Med. 2025 Jul;211(7):1156-1164.
Dixon KJ. Pathophysiology of traumatic brain injury. Phys Med Rehabil Clin N Am. 2017;28(2):215-225.
Gibbs KW, Semler MW, Driver BE, et al. Noninvasive ventilation for preoxygenation during emergency intubation. N Engl J Med. 2024;390(23):2165-2177.
Godoy DA, Badenes R, Murillo-Cabezas F. Ten physiological commandments for severe head injury. Rev Esp Anestesiol Reanim (Engl Ed). 2021;68(5):280-292.
Godoy DA, Murillo-Cabezas F, Suarez JI, Badenes R, Pelosi P, Robba C. "THE MANTLE" bundle for minimizing cerebral hypoxia in severe traumatic brain injury. Crit Care. 2023;27(1):13.
Hawryluk GWJ, Lulla A, Bell R, et al. Guidelines for prehospital management of traumatic brain injury 3rd edition: executive summary. Neurosurgery. 2023;93(6):e159-e169.
Hoiland RL, Fisher JA, Ainslie PN. Regulation of the cerebral circulation by arterial carbon dioxide. Compr Physiol. 2019;9(3):1101-1154.
Hoyne J, Edlow J. Airway management in patients with acute brain injury or ischemia. J Emerg Med. 2025 Jan 6.
Hu Q, Liu X, Xu T, Wen C, Liu L, Feng J. The impact of ketamine on emergency rapid sequence intubation: a systematic review and meta-analysis. BMC Emerg Med. 2024;24(1):174.
Karamchandani K, Nasa P, Jarzebowski M, et al. Tracheal intubation in critically ill adults with a physiologically difficult airway: an international Delphi study. Intensive Care Med. 2024;50(10):1563-1579.
Kotani Y, Pruna A, Turi S, et al. Propofol and survival: an updated meta-analysis of randomized clinical trials. Crit Care. 2023;27:139.
Liu CC, Chen IW, Liu PH, et al. Efficacy of propofol-based anesthesia against risk of brain swelling during craniotomy: a meta-analysis of randomized controlled studies. J Clin Anesth. 2024;92:111306.
Lundstrom LH, Duez CH, Norskov AK, Rosenstock CV, Thomsen JL, Moller AM, et al. Avoidance versus use of neuromuscular blocking agents for improving conditions during tracheal intubation or direct laryngoscopy in adults and adolescents. Cochrane Database Syst Rev. 2017;5:CD009237.
Mascia L, Fanelli V, Mistretta A, et al. Lung-protective mechanical ventilation in patients with severe acute brain injury: a multicenter randomized clinical trial (PROLABI). Am J Respir Crit Care Med. 2024;210(9):1123-1131.
Muhs AL, Seitz KP, Qian ET, et al. Video vs direct laryngoscopy for tracheal intubation after cardiac arrest: a secondary analysis of the Direct vs Video Laryngoscope Trial. Chest. 2025;167(5):1408-1415.
Ng SY, Lee AYW. Traumatic brain injuries: pathophysiology and potential therapeutic targets. Front Cell Neurosci. 2019;13:528.
Okasha AS, Fayed AM, Saleh AS. The FOUR score predicts mortality, endotracheal intubation and ICU length of stay after traumatic brain injury. Neurocrit Care. 2014;21:496-504.
Okyay RD, Küçükosman G, Köksal BG, et al. Effects of supraglottic airway devices on hemodynamic response and optic nerve sheath diameter: Proseal LMA, LMA Supreme, and I-gel LMA. Medicina (Kaunas). 2023;59(4):753.
Ottolenghi S, Sabbatini G, Brizzolari A, Samaja M, Chiumello D. Hyperoxia and oxidative stress in anesthesia and critical care medicine. Minerva Anestesiol. 2020;86(1):64-75.
Pitre T, Liu W, Zeraatkar D, Casey JD, Dionne JC, Gibbs KW, et al. Preoxygenation strategies for intubation of patients who are critically ill: a systematic review and network meta-analysis of randomised trials. Lancet Respir Med. 2025.
Rajajee V, Riggs B, Seder DB. Emergency neurological life support: airway, ventilation, and sedation. Neurocrit Care. 2017;27:4-28.
Renew JR, Ratzlaff R, Hernandez-Torres V, et al. Neuromuscular blockade management in the critically ill patient. J Intensive Care. 2020;8:37.
Robba C, Battaglini D, Abbas A, et al. Clinical practice and effect of carbon dioxide on outcomes in mechanically ventilated acute brain-injured patients. Intensive Care Med. 2024;50(2):234-246. Published correction appears in Intensive Care Med. 2024;50(2):317-318.
Robba C, Giardiello D, Almondo C, et al. Ventilation practices in acute brain injured patients and association with outcomes: the VENTIBRAIN multicenter observational study. Intensive Care Med. 2025;51(2):318-331.
Rotheray KR, et al. What is the relationship between the Glasgow coma scale and airway protective reflexes in the Chinese population? Resuscitation. 2012;83(1):86-89.
Russell DW, Casey JD, Gibbs KW, et al. Effect of fluid bolus administration on cardiovascular collapse among critically ill patients undergoing tracheal intubation: a randomized clinical trial. JAMA. 2022;328(3):270-279.
Russotto V, Myatra SN, Laffey JG, et al. Intubation practices and adverse peri-intubation events in critically ill patients from 29 countries. JAMA. 2021;325(12):1164-1172. Published correction appears in JAMA. 2021;325(24):2507.
Sanfilippo F, Santonocito C, Veenith T, et al. The role of neuromuscular blockade in patients with traumatic brain injury: a systematic review. Neurocrit Care. 2015;22:325-334.
Shafique MA, Haseeb A, Asghar B, et al. Assessing the impact of pre-hospital airway management on severe traumatic brain injury: a systematic review and meta-analysis. Am J Emerg Med. 2024;78:188-195.
Soto-Páramo DG, Pérez-Nieto OR, Deloya-Tomas E, et al. Fisiopatología, diagnóstico y tratamiento de la lesión cerebral traumática. Rev Neurol Neurocir Psiquiat. 2022;50(1):4-15.
Taccone FS, De Oliveira Manoel AL, Robba C, et al. Use a “GHOST-CAP” in acute brain injury. Crit Care. 2020;24:89.
Teasdale G, Maas A, Lecky F, Manley G, Stocchetti N, Murray G. The Glasgow Coma Scale at 40 years: standing the test of time. Lancet Neurol. 2014;13(8):844-854. Published correction appears in Lancet Neurol. 2014;13(9):863.
Thapa K, Khan H, Singh TG, Kaur A. Traumatic brain injury: mechanistic insight on pathophysiology and potential therapeutic targets. J Mol Neurosci. 2021;71(9):1725-1742.
von Hellmann R, Fuhr N, Ward A Maia I, et al. Effect of bougie use on first-attempt success in tracheal intubations: a systematic review and meta-analysis. Ann Emerg Med. 2024;83(2):132-144.
Wiener J, McIntyre A, Janzen S, et al. Opioids and cerebral physiology in the acute management of traumatic brain injury: a systematic review. Brain Inj. 2019;33(5):559-566.
Wilcox SR, Bittner EA, Elmer J, Seigel TA, Nguyen NT, Dhillon A, et al. Neuromuscular blocking agent administration for emergent tracheal intubation is associated with decreased prevalence of procedure-related complications. Crit Care Med. 2012;40(6):1808-1813.
Zeiler FA, Teitelbaum J, West M, Gillman LM. The ketamine effect on ICP in traumatic brain injury. Neurocrit Care. 2014;21(1):163-173.