Research
Non-drug perioperative interventions to reduce postoperative pulmonary complications after abdominal surgery: systematic review and meta-analysis
Chanyan Huang, Xu Zhao, Siyu Geng, et al
BMJ 2026; 393 doi: https://doi.org/10.1136/bmj-2025-089001 (Published 09 April 2026)Cite this as: BMJ 2026;393:e089001
Abstract
Objective To evaluate the effectiveness of perioperative non-drug interventions in reducing postoperative pulmonary complications (PPCs) in adults undergoing abdominal surgery.
Design Systematic review and meta-analysis.
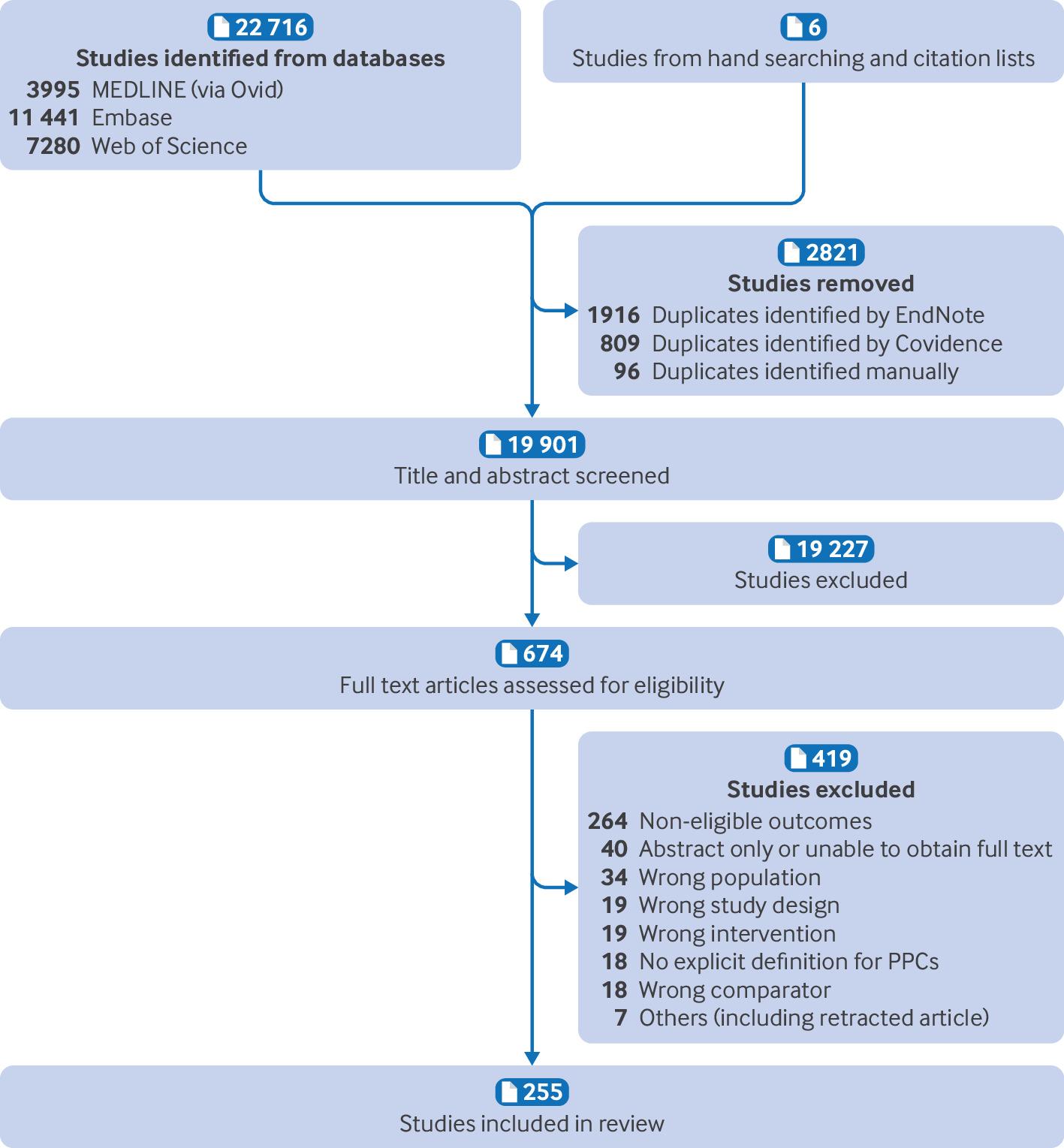
Data sources Ovid MEDLINE, Embase, and Web of Science from database inception to January 2025 and updated in January 2026, with no language restrictions.
Study selection Randomised controlled trials assessing the effectiveness of perioperative non-drug interventions for the prevention of PPCs in adults undergoing elective abdominal surgery under general anaesthesia, with clearly defined PPCs.
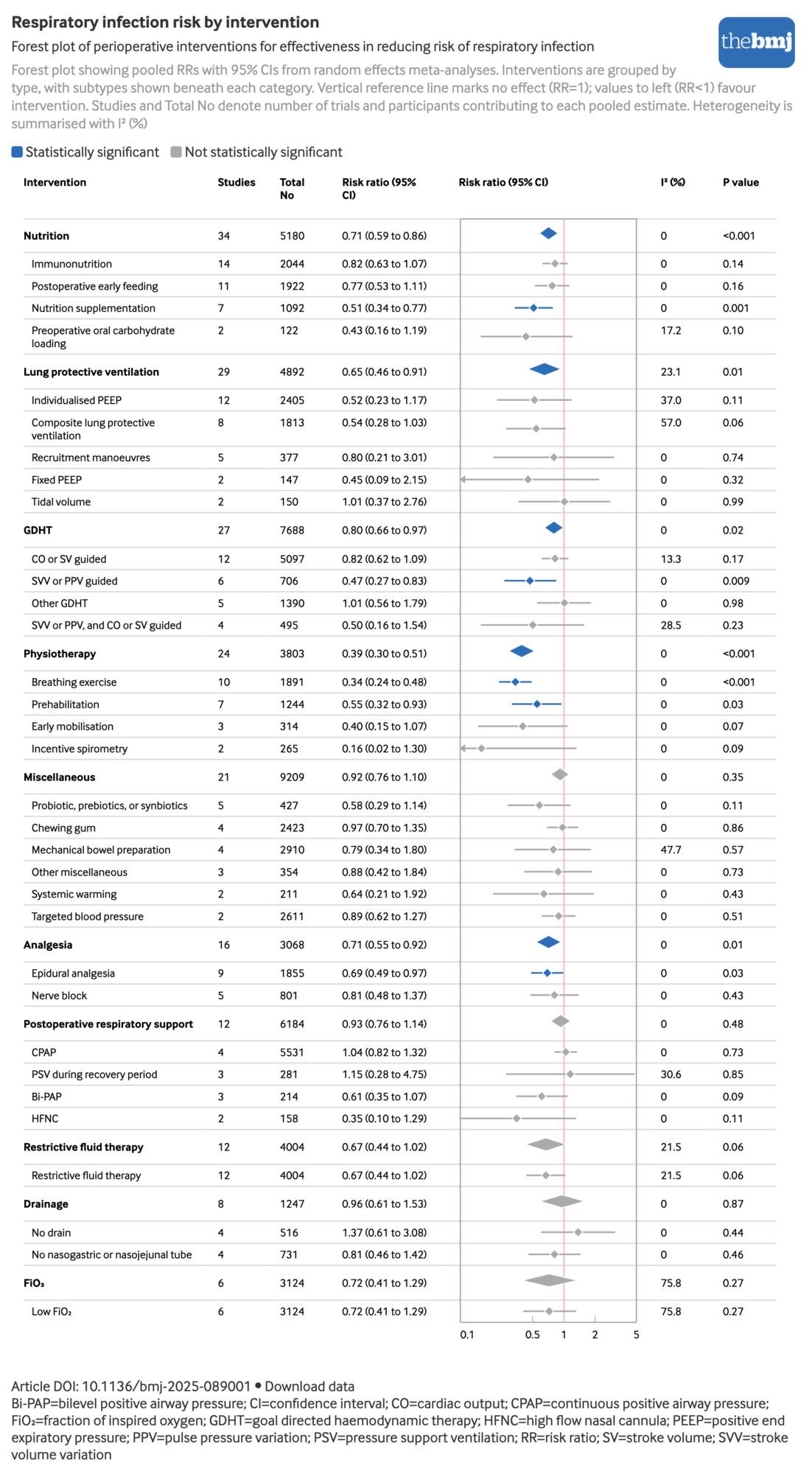
Main outcome measures The primary outcome was the proportion of patients developing PPCs. Secondary outcomes included the proportion of patients with PPC subtypes according to European Perioperative Clinical Outcome definitions (respiratory infection, respiratory failure, pleural effusion, atelectasis, or pneumothorax) and hospital length of stay.
Data extraction and synthesis Two reviewers independently screened studies, extracted data, and assessed risk of bias with the Cochrane RoB 2.0 tool. Data were synthesised using meta-analyses and trial sequential analyses, with the evidence certainty assessed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach.
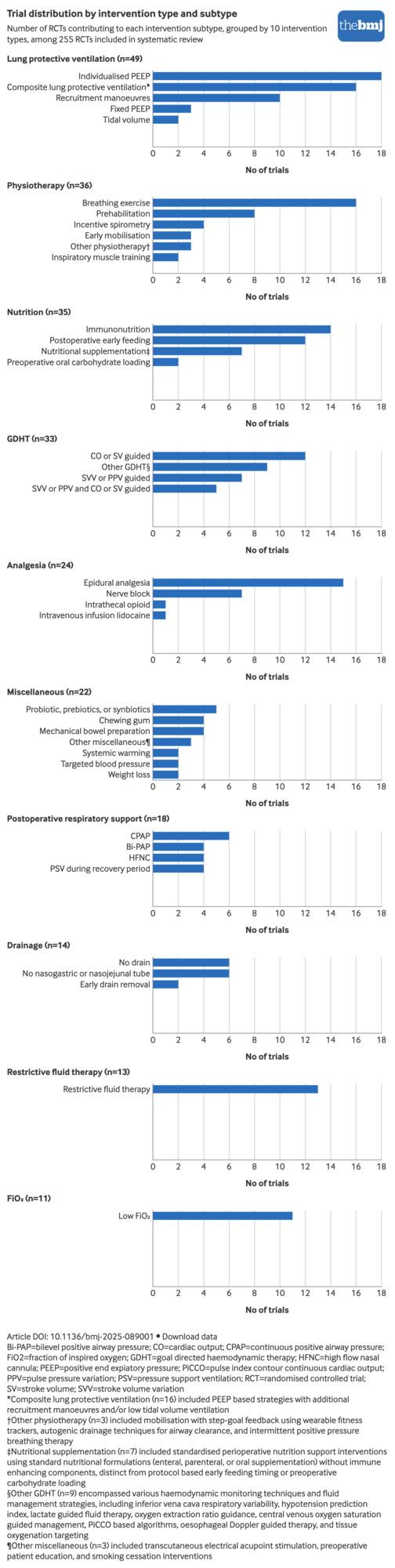
Results 255 trials including 55 260 participants were included, evaluating 10 types of interventions with 39 subtypes for PPC prevention. PPCs occurred in 6467 (11.7%) participants across all included trials. High certainty evidence showed that low fraction of inspired oxygen (FiO2) significantly reduced PPCs (risk ratio 0.81, 95% confidence interval 0.71 to 0.92). Moderate certainty evidence showed benefit for four intervention types: lung protective ventilation (risk ratio 0.66, 0.57 to 0.76), physiotherapy (0.55, 0.46 to 0.65), analgesia (0.73, 0.64 to 0.84), and nutrition (0.74, 0.63 to 0.87), with individualised positive end expiratory pressure, composite lung protective ventilation, early mobilisation, and epidural analgesia also showing benefit at the subtype level. Trial sequential analysis confirmed sufficient cumulative evidence for all the above interventions except early mobilisation. By contrast, goal directed haemodynamic therapy, targeted blood pressure management, restrictive fluid therapy, and postoperative bi-level positive airway pressure showed no evidence of benefit, with moderate certainty.
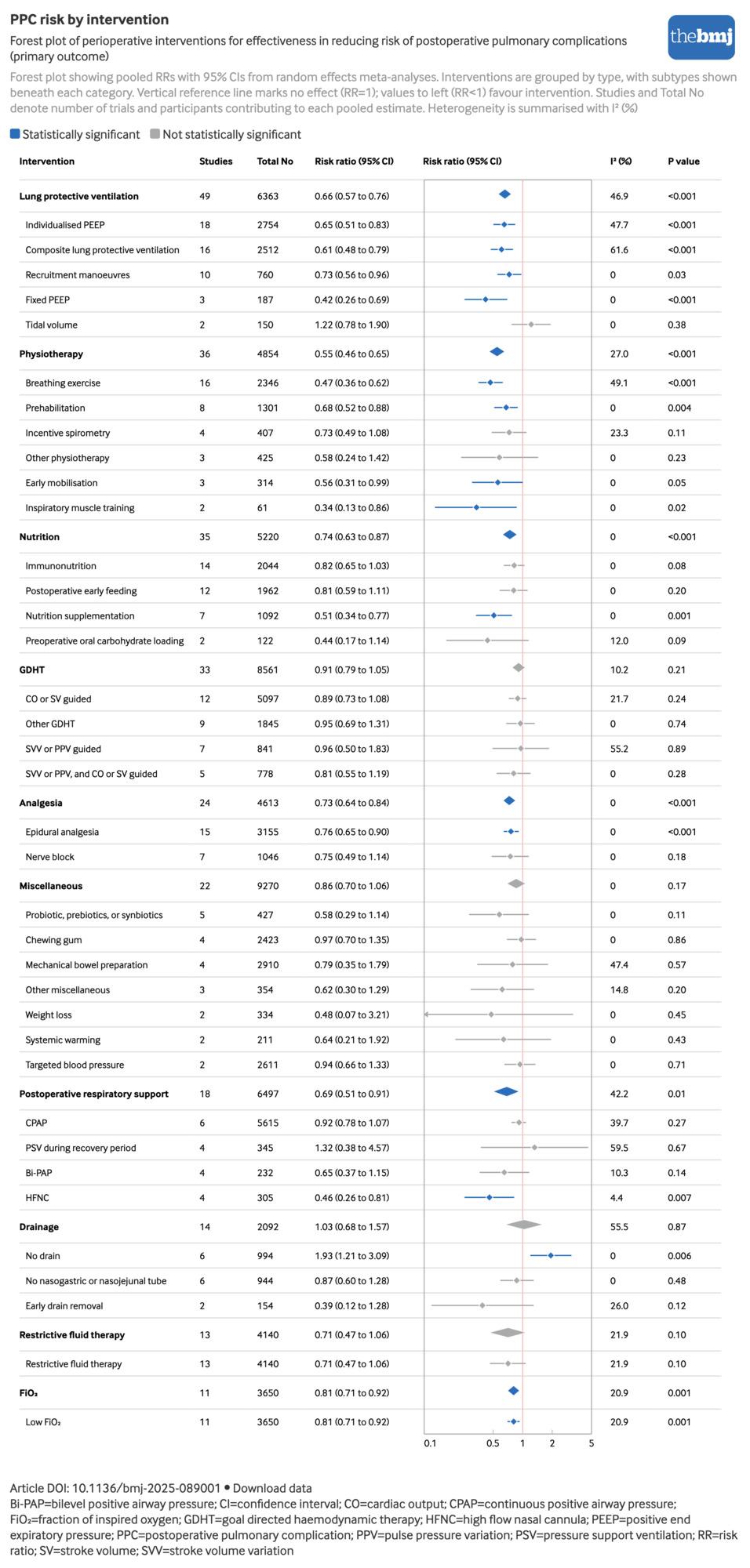
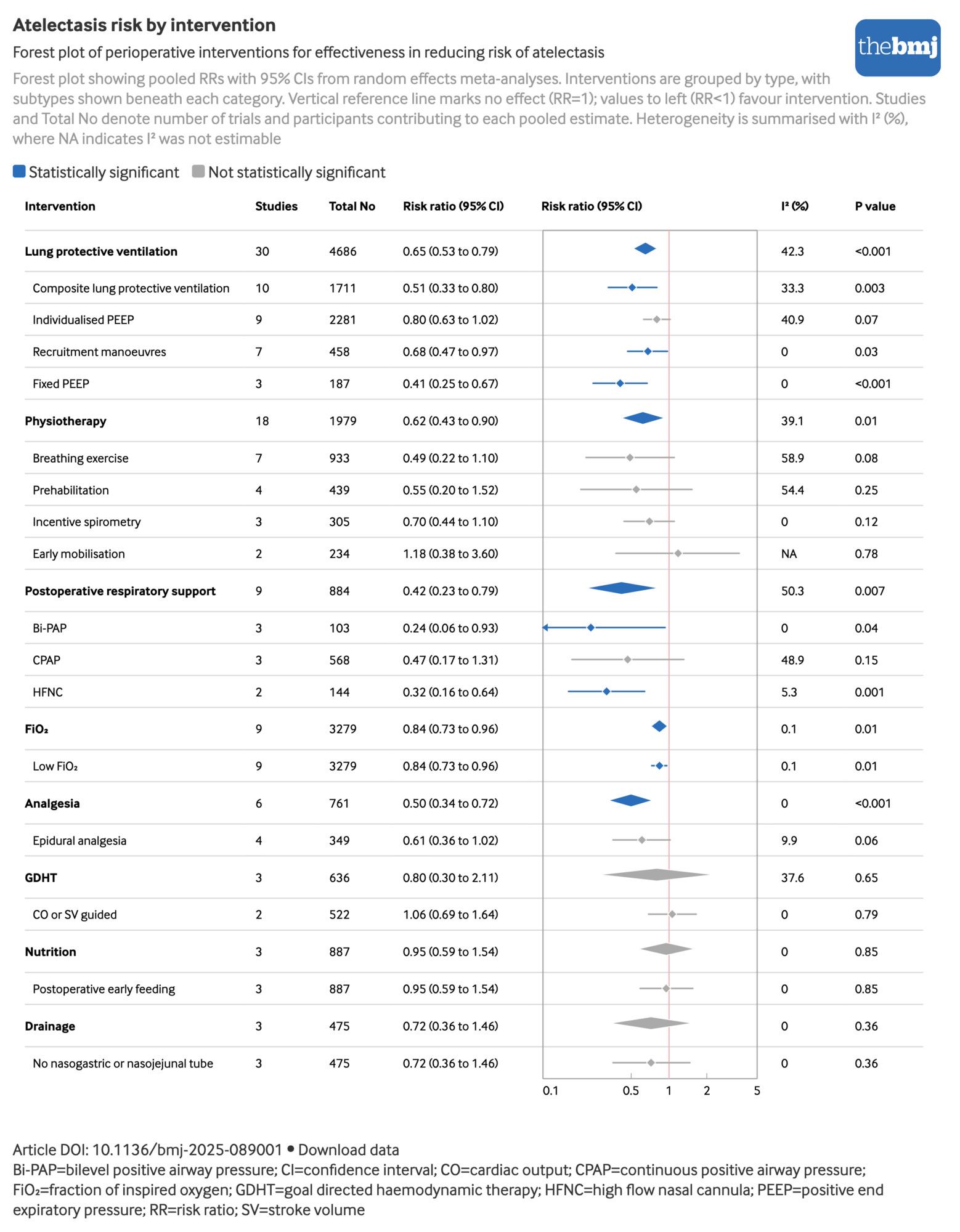
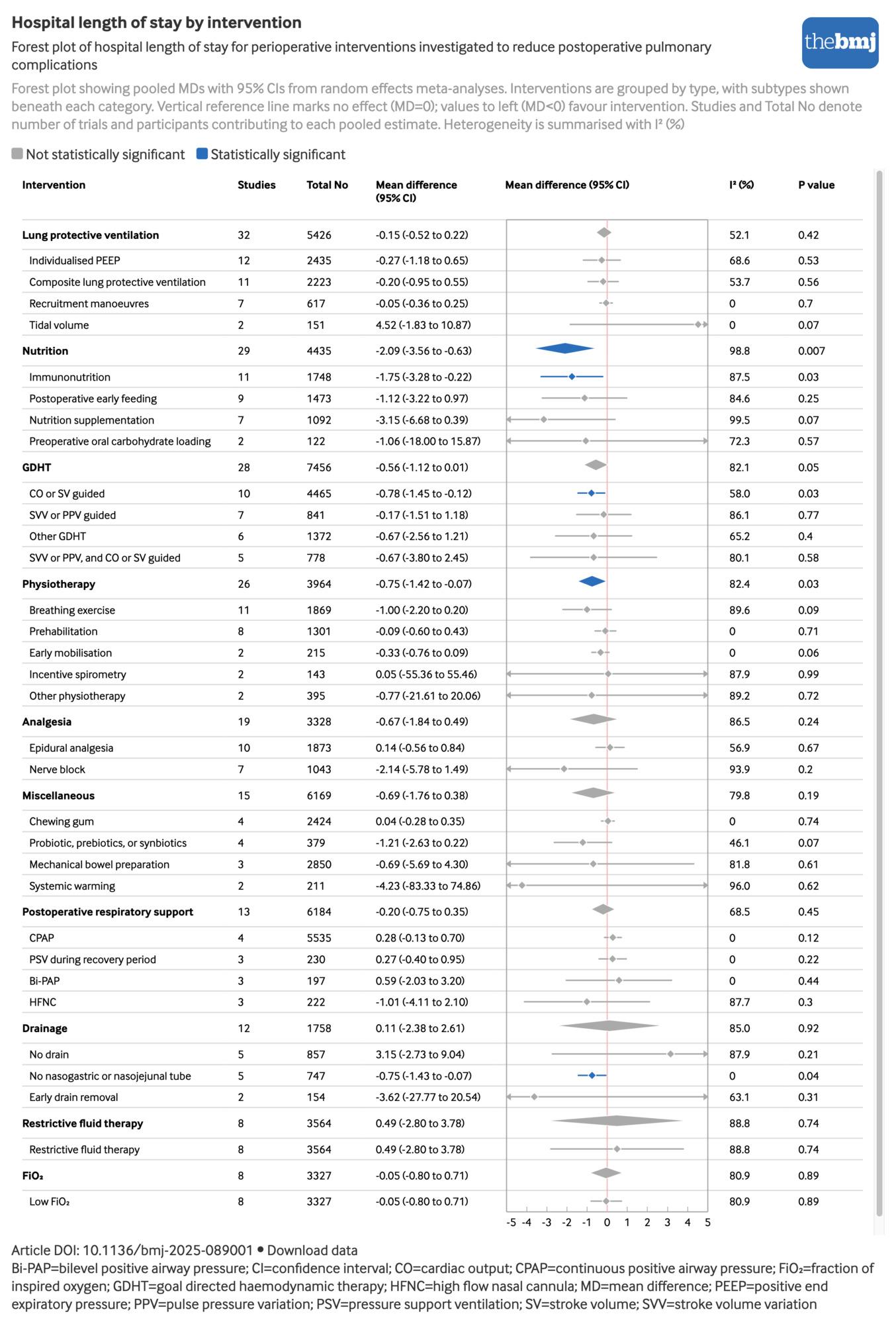
Conclusions This synthesis establishes an evidence hierarchy for PPC prevention in abdominal surgery. Low FiO2 is the only intervention supported by high certainty evidence and should be prioritised in clinical practice. Other beneficial strategies include lung protective ventilation, physiotherapy, analgesic techniques, and nutrition interventions. Conversely, the role of goal directed haemodynamic therapy—despite its widespread use—warrants reconsideration for PPC prevention. These findings facilitate prioritisation of effective interventions and development of evidence based guidelines.
Study registration PROSPERO CRD42025637449.