JOURNAL ARTICLE
Aspergillosis-Attributable Mortality in the United States: Analysis of Death Certificate Data
Thomas J Walsh, Dakota Sicignano, Matthew Mastropietro, et al
Clinical Infectious Diseases, Volume 82, Issue 1, 15 January 2026, Pages 86–92, https://doi.org/10.1093/cid/ciaf653
Abstract
Background
The nationwide attributable mortality of aspergillosis in the era of mold-active triazoles is poorly understood.
Methods
We analyzed data from the US National Vital Statistics System for 2018-2024. Aspergillosis-attributable mortality was identified using an International Classification of Diseases-10th Revision (ICD-10) diagnosis code of B44.x listed anywhere on the death certificate. We present age-adjusted mortality rates (AAMRs)/1 000 000 persons with 95% confidence intervals (CIs) for aspergillosis deaths and stratified by demographics. Risk ratios (RRs) were used to compare AAMRs across strata and the proportion of key comorbidities included on aspergillosis versus non-aspergillosis certificates.
Results
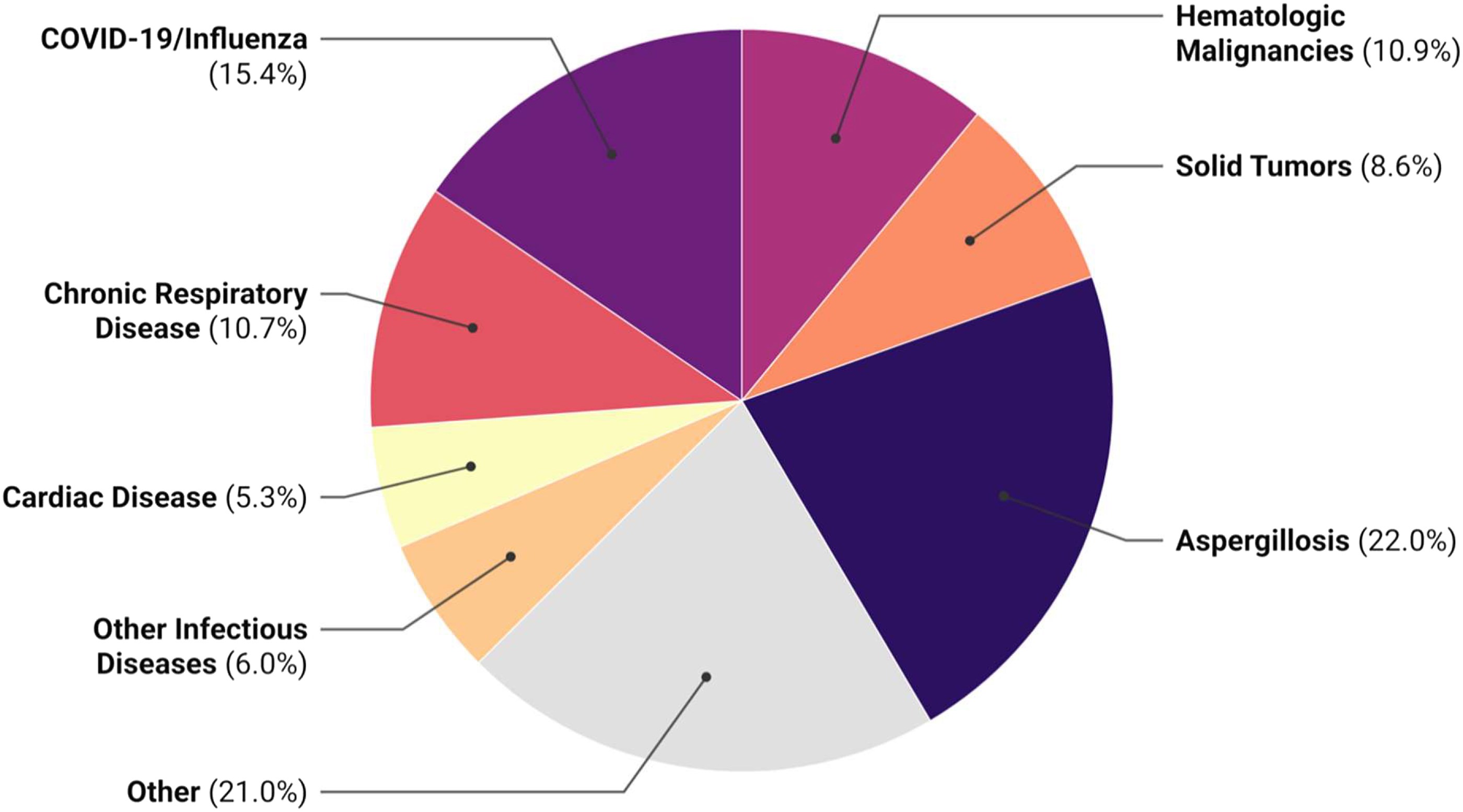
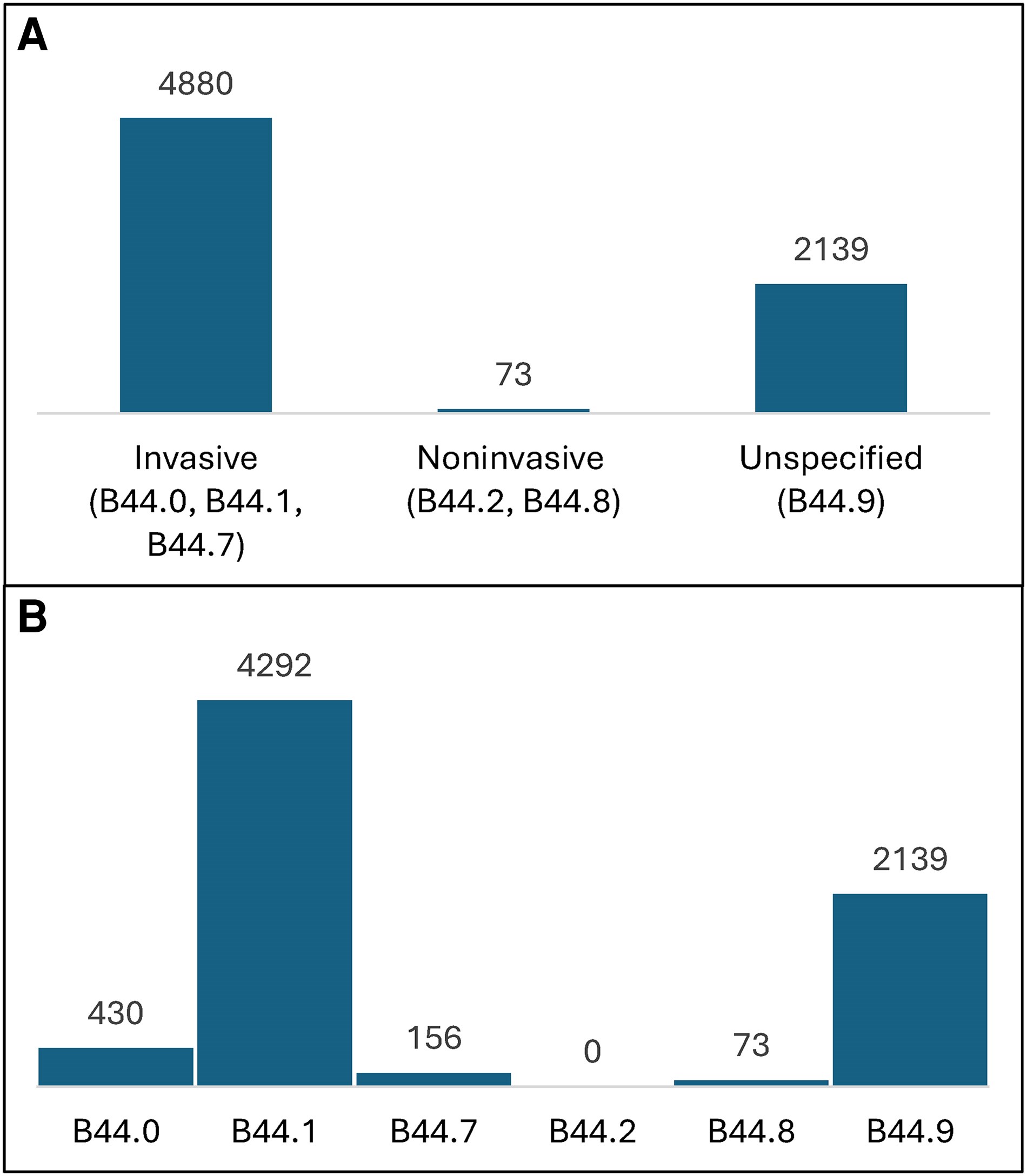
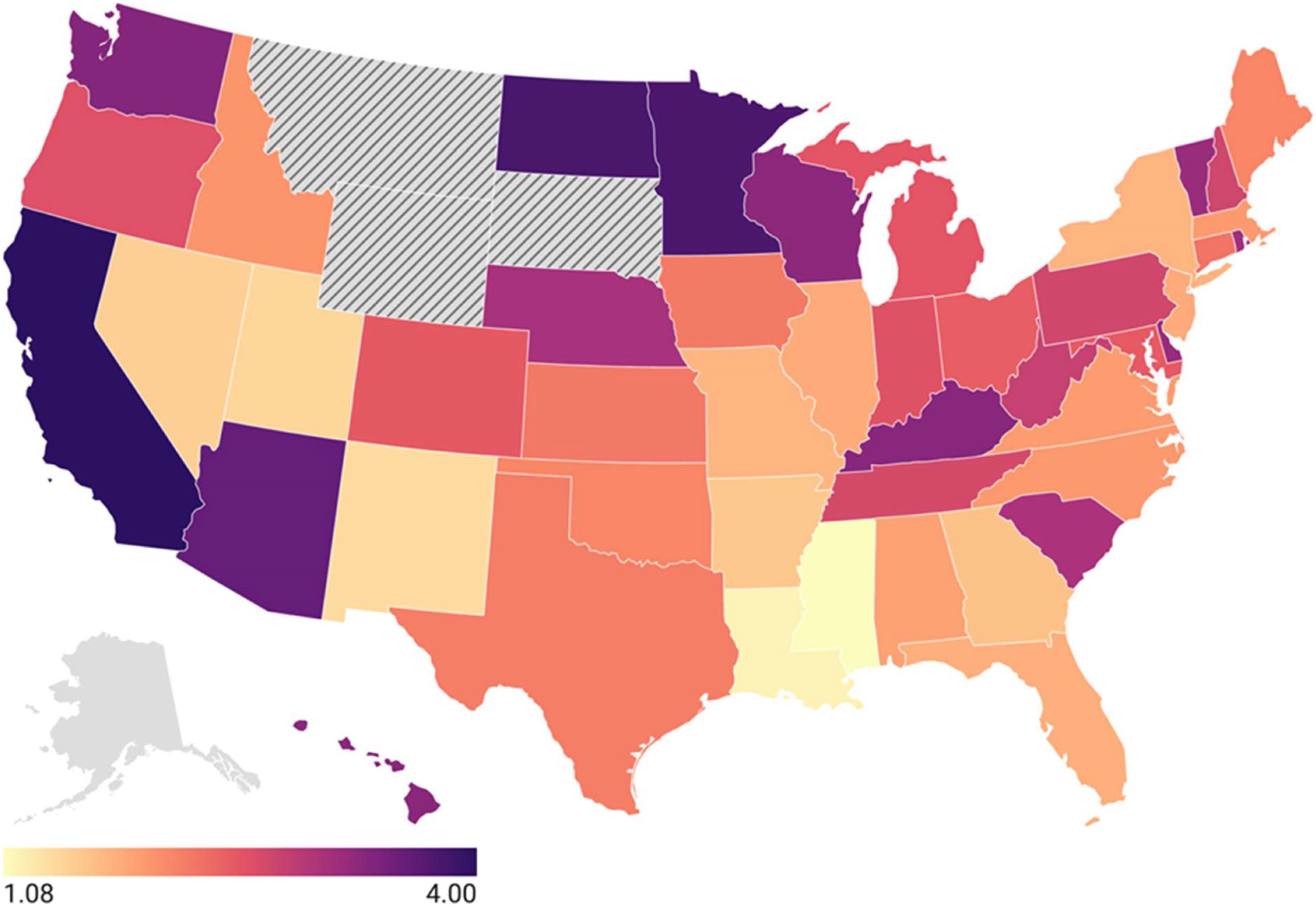
There were 7063 aspergillosis-attributable deaths identified (AAMR: 2.43, 2.37-2.49). Of these, 1551 (22.0%) of death certificates had aspergillosis listed as the primary cause. An invasive aspergillosis (IA) disease code was most often listed (n = 4880 certificates); specifically, “other pulmonary aspergillosis” (B44.1, n = 4292 certificates). Unspecified aspergillosis was listed on 2139 death certificates. Non-IA codes were rarely observed (n = 73 certificates). Aspergillosis deaths increased in later years of analysis (AAMR range: 2.50-3.01) versus 2018-2020 (AAMR: 2.01). Nearly 60% of aspergillosis deaths occurred in those ≥65-years-old, and the AAMR was higher in males (RR: 1.64, 1.50-1.80). Neither race nor ethnicity was associated with differences in AAMR. AAMRs varied across states.
Conclusions
Among patients with a death certificate with aspergillosis, primary attributable mortality was 22.0%. Our results may be useful as experts seek to better understand the true epidemiology of IA, develop efforts to raise disease awareness, and reduce IA-related mortality.