- Guidelines
- Open Access
- Published:
The European guideline on management of major bleeding and coagulopathy following trauma: sixth edition
Rolf Rossaint, Arash Afshari, Bertil Bouillon, et al
Crit Care 2023; 27: 80
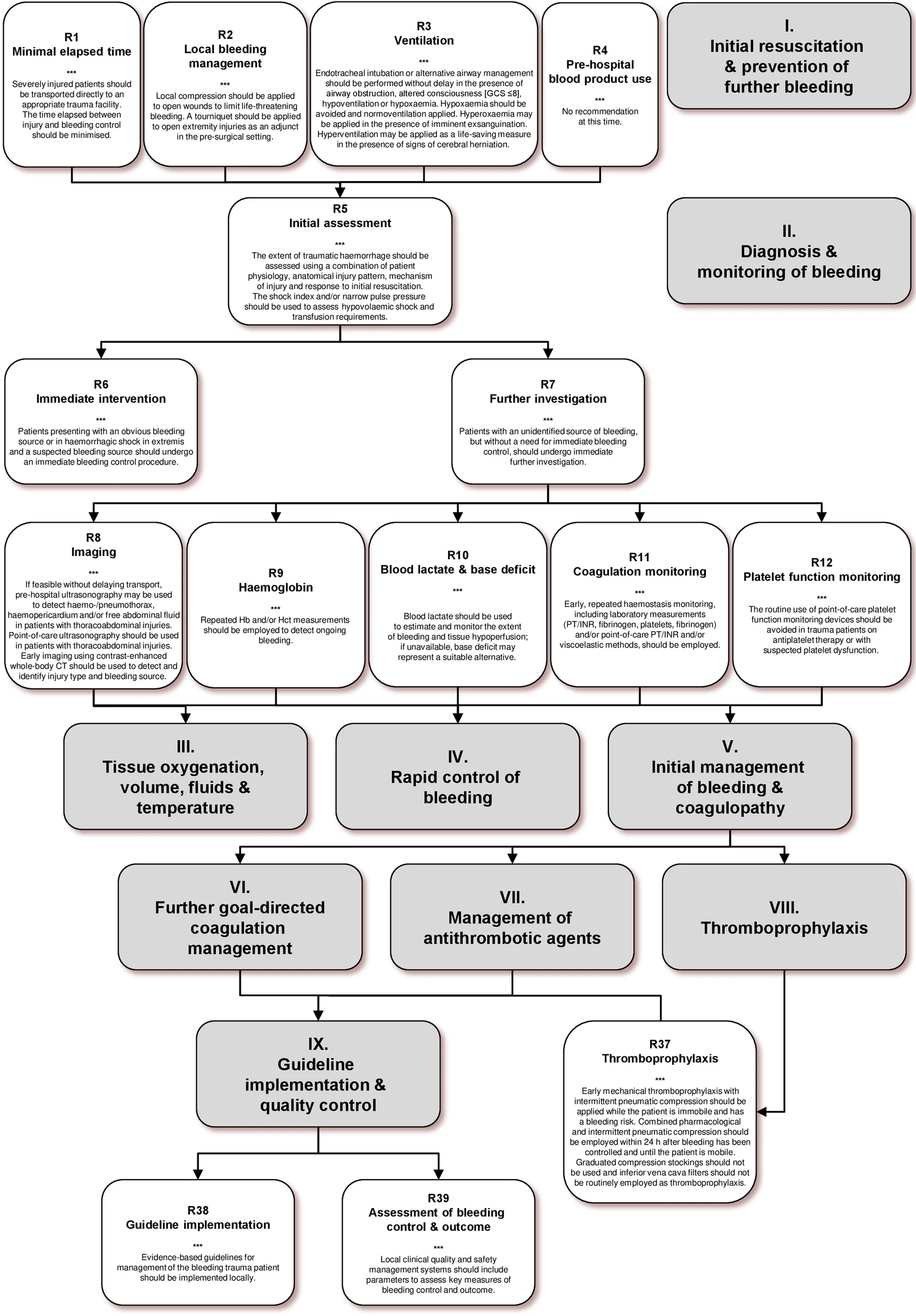
I. Initial resuscitation and prevention of further bleeding
Minimal elapsed time
Recommendation 1
We recommend that severely injured patients be transported directly to an appropriate trauma facility (Grade 1B).
We recommend that the time elapsed between injury and bleeding control be minimised (Grade 1B).
Local bleeding management
Recommendation 2
We recommend local compression of open wounds to limit life-threatening bleeding (Grade 1B).
We recommend adjunct tourniquet use to stop life-threatening bleeding from open extremity injuries in the pre-surgical setting (Grade 1B).
Ventilation
Recommendation 3
We recommend that endotracheal intubation or alternative airway management be performed without delay in the presence of airway obstruction, altered consciousness [Glasgow Coma Scale (GCS) ≤ 8], hypoventilation or hypoxaemia (Grade 1B).
We recommend the avoidance of hypoxaemia (Grade 1A).
We suggest the avoidance of hyperoxaemia, except in the presence of imminent exsanguination (Grade 2B).
We recommend normoventilation of trauma patients (Grade 1B).
We suggest hyperventilation as a life-saving measure in the presence of signs of cerebral herniation (Grade 2C).
Pre-hospital blood product use
Recommendation 4
No clear recommendation or suggestion in favour or against the use of pre-hospital blood products can be provided at this time.
II. Diagnosis and monitoring of bleeding
Initial assessment
Recommendation 5
We recommend that the physician clinically assess the extent of traumatic haemorrhage using a combination of patient physiology, anatomical injury pattern, mechanism of injury and the patient response to initial resuscitation (Grade 1C).
We recommend that the shock index (SI) and/or pulse pressure (PP) be used to assess the degree of hypovolaemic shock and transfusion requirements (Grade 1C).
Immediate intervention
Recommendation 6
We recommend that patients with an obvious bleeding source and those presenting with haemorrhagic shock in extremis and a suspected source of bleeding undergo an immediate bleeding control procedure (Grade 1B).
Further investigation
Recommendation 7
We recommend that patients with an unidentified source of bleeding, but without a need for immediate bleeding control, undergo immediate further investigation to determine the bleeding source (Grade 1C).
Imaging
Recommendation 8
We suggest the use of pre-hospital ultrasonography (PHUS) for the detection of haemo-/pneumothorax, haemopericardium and/or free abdominal fluid in patients with thoracoabdominal injuries, if feasible without delaying transport (Grade 2B).
We recommend the use of point-of-care ultrasonography (POCUS), including FAST, in patients with thoracoabdominal injuries (Grade 1C).
We recommend early imaging using contrast-enhanced whole-body CT (WBCT) for the detection and identification of the type of injury and the potential source of bleeding (Grade 1B).
Haemoglobin
Recommendation 9
We recommend the use of repeated Hb and/or Hct measurements as a laboratory marker for bleeding, as an initial value in the normal range may mask early-phase bleeding (Grade 1B).
Blood lactate and base deficit
Recommendation 10
We recommend blood lactate as a sensitive test to estimate and monitor the extent of bleeding and tissue hypoperfusion; in the absence of lactate measurements, base deficit may represent a suitable alternative (Grade 1B).
Coagulation monitoring
Recommendation 11
We recommend the early and repeated monitoring of haemostasis, using either a traditional laboratory determination such as prothrombin time (PT)/international normalised ratio (INR), Clauss fibrinogen level and platelet count and/or point-of-care (POC) PT/INR and/or a viscoelastic method (Grade 1C).
Platelet function monitoring
Recommendation 12
We recommend that the routine use of POC platelet function devices for platelet function monitoring in trauma patients on antiplatelet therapy or with suspected platelet dysfunction be avoided (Grade 1C).
III. Tissue oxygenation, volume, fluids and temperature
Volume replacement and target blood pressure
Recommendation 13
In the initial phase following trauma, we recommend the use of a restricted volume replacement strategy with a target systolic blood pressure of 80–90 mmHg (mean arterial pressure 50–60 mmHg) until major bleeding has been stopped without clinical evidence of brain injury (Grade 1B).
In patients with severe TBI (GCS ≤ 8), we recommend that a mean arterial pressure ≥ 80 mmHg be maintained (Grade 1C).
Vasopressors and inotropic agents
Recommendation 14
If a restricted volume replacement strategy does not achieve the target blood pressure, we recommend the administration of noradrenaline in addition to fluids to maintain target arterial pressure (Grade 1C).
We recommend infusion of dobutamine in the presence of myocardial dysfunction (Grade 1C).
Type of fluid
Recommendation 15
We recommend that fluid therapy using a 0.9% sodium chloride or balanced crystalloid solution be initiated in the hypotensive bleeding trauma patient (Grade 1B).
We recommend that hypotonic solutions such as Ringer’s lactate be avoided in patients with severe head trauma (Grade 1B).
We recommend that the use of colloids be restricted due to the adverse effects on haemostasis (Grade 1C).
Erythrocytes
Recommendation 16
If erythrocyte transfusion is necessary, we recommend a target haemoglobin of 70–90 g/L (Grade 1C).
Cell salvage
Recommendation 17
We suggest that cell salvage be considered in the presence of severe bleeding from an abdominal, pelvic or thoracic cavity (Grade 2B).
Temperature management
Recommendation 18
We recommend early application of measures to reduce heat loss and warm the hypothermic patient to achieve and maintain normothermia (Grade 1C).
IV. Rapid control of bleeding
Damage control surgery
Recommendation 19
We recommend damage control surgery in the severely injured patient presenting with haemorrhagic shock, signs of ongoing bleeding, coagulopathy and/or combined abdominal vascular and pancreatic injuries (Grade 1B).
Other factors that should trigger a damage control approach are hypothermia, acidosis, inaccessible major anatomic injury, a need for time-consuming procedures (Grade 1C).
We recommend primary definitive surgical management in the absence of any of the factors above (Grade 1C).
Pelvic ring closure and stabilisation
Recommendation 20
We recommend the adjunct use of a pelvic binder in the pre-hospital setting to limit life-threatening bleeding in the presence of a suspected pelvic fracture (Grade 1C).
We recommend that patients with pelvic ring disruption in haemorrhagic shock undergo pelvic ring closure and stabilisation as early as possible (Grade 1B).
Embolisation, packing, surgery and resuscitative endovascular balloon occlusion of the aorta (REBOA)
Recommendation 21
We recommend temporary extra-peritoneal packing when bleeding is ongoing and/or when angioembolisation cannot be achieved in a timely manner. Extra-peritoneal packing can be combined with open abdominal surgery when necessary (Grade 1C).
We suggest that REBOA be considered in patients with noncompressible life-threatening traumatic haemorrhage to bridge the gap between haemodynamic collapse and haemorrhage control (Grade 2C).
Local haemostatic measures
Recommendation 22
We recommend the use of topical haemostatic agents in combination with other surgical measures or with packing for venous or moderate arterial bleeding associated with parenchymal injuries (Grade 1B).
V. Initial management of bleeding and coagulopathy
Antifibrinolytic agents
Recommendation 23
We recommend that tranexamic acid (TXA) be administered to the trauma patient who is bleeding or at risk of significant bleeding as soon as possible, if feasible en route to the hospital, and within 3 h after injury at a loading dose of 1 g infused over 10 min, followed by an i.v. infusion of 1 g over 8 h (Grade 1A).
We recommend that the administration of TXA not await results from a viscoelastic assessment (Grade 1B).
Coagulation support
Recommendation 24
We recommend that monitoring and measures to support coagulation be initiated immediately upon hospital admission (Grade 1B).
Initial coagulation resuscitation
Recommendation 25
In the initial management of patients with expected massive haemorrhage, we recommend one of the two following strategies:
- Fibrinogen concentrate or cryoprecipitate and pRBC (Grade 1C)
- FFP or pathogen-inactivated FFP in a FFP/pRBC ratio of at least 1:2 as needed (Grade 1C)
In addition, we suggest a high platelet/pRBC ratio (Grade 2B).
VI. Further goal-directed coagulation management
Goal-directed therapy
Recommendation 26
We recommend that resuscitation measures be continued using a goal-directed strategy, guided by standard laboratory coagulation values and/or VEM (Grade 1B).
Fresh frozen plasma-based management
Recommendation 27
If a FFP-based coagulation resuscitation strategy is used, we recommend that further use of FFP be guided by standard laboratory coagulation screening parameters (PT and/or APTT > 1.5 times normal and/or viscoelastic evidence of a coagulation factor deficiency) (Grade 1C).
We recommend that the use of FFP be avoided for the correction of hypofibrinogenemia if fibrinogen concentrate and/or cryoprecipitate are available (Grade 1C).
Coagulation factor concentrate-based management
Recommendation 28
If a CFC-based strategy is used, we recommend treatment with factor concentrates based on standard laboratory coagulation parameters and/or viscoelastic evidence of a functional coagulation factor deficiency (Grade 1C).
Provided that fibrinogen levels are normal, we suggest that prothrombin complex concentrate (PCC) is administered to the bleeding patient based on evidence of delayed coagulation initiation using VEM (Grade 2C).
We suggest that monitoring of FXIII be included in coagulation support algorithms and that FXIII be supplemented in bleeding patients with a functional FXIII deficiency (Grade 2C).
Fibrinogen supplementation
Recommendation 29
We recommend treatment with fibrinogen concentrate or cryoprecipitate if major bleeding is accompanied by hypofibrinogenemia (viscoelastic signs of a functional fibrinogen deficit or a plasma Clauss fibrinogen level ≤ 1.5 g/L) (Grade 1C)*
We suggest an initial fibrinogen supplementation of 3–4 g. This is equivalent to 15–20 single donor units of cryoprecipitate or 3–4 g fibrinogen concentrate. Repeat doses should be guided by VEM and laboratory assessment of fibrinogen levels (Grade 2C).
Platelets
Recommendation 30
We suggest that platelets be administered to maintain a platelet count above 50 × 109/L in trauma patients with ongoing bleeding and above 100 × 109/L in patients with TBI (Grade 2C).
If administered, we suggest an initial dose of four to eight single platelet units or one aphaeresis pack (Grade 2B).
Calcium
Recommendation 31
We recommend that ionised calcium levels be monitored and maintained within the normal range following major trauma and especially during massive transfusion (Grade 1C).
We recommend the administration of calcium chloride to correct hypocalcaemia (Grade 1C).
Recombinant activated coagulation factor VII
Recommendation 32
We do not recommend the use of recombinant activated coagulation factor VII (rFVIIa) as first-line treatment (Grade 1B).
We suggest that the off-label use of rFVIIa be considered only if major bleeding and traumatic coagulopathy persist despite all other attempts to control bleeding, systemic homeostasis and best-practice use of conventional haemostatic measures (Grade 2C).
VII. Management of antithrombotic agents
Reversal of vitamin K-dependent oral anticoagulants
Recommendation 33
In the bleeding trauma patient, we recommend the emergency reversal of vitamin K-dependent oral anticoagulants with the early use of both PCC and 5–10 mg i.v. phytomenadione (vitamin K1) (Grade 1A).
Management of direct oral anticoagulants—factor Xa inhibitors
Recommendation 34
We suggest the measurement of plasma levels of oral direct antifactor Xa agents such as apixaban, edoxaban or rivaroxaban in patients treated or suspected of being treated with one of these agents (Grade 2C).
We suggest that measurement of anti-Xa activity be calibrated for the specific agent. If not possible or available, we suggest low molecular weight heparin (LMWH)-calibrated anti-Xa assays as a reliable alternative (Grade 2C).
If bleeding is life-threatening in the presence of an apixaban or rivaroxaban effect, especially in patients with TBI, we suggest reversal with andexanet alfa (Grade 2C).
If andexanet alfa is not available, or in patients receiving edoxaban, we suggest the administration of PCC (25–50 U/kg) (Grade 2C).
Management of direct oral anticoagulants—direct thrombin inhibitors
Recommendation 35
We suggest the measurement of dabigatran plasma levels using diluted thrombin time in patients treated or suspected of being treated with dabigatran (Grade 2C).
If measurement is not possible or available, we suggest measurement of the standard thrombin time to allow a qualitative estimation of the presence of dabigatran (Grade 2C).
If bleeding is life-threatening in those receiving dabigatran, we recommend treatment with idarucizumab (i.v. 5 g) (Grade 1C).
Antiplatelet agents
Recommendation 36
We recommend that routine platelet transfusion be avoided in patients with ongoing bleeding who have been treated with APAs (Grade 1C).
VIII. Thromboprophylaxis
Thromboprophylaxis
Recommendation 37
We recommend early initiation of mechanical thromboprophylaxis with intermittent pneumatic compression (IPC) while the patient is immobile and has a bleeding risk (Grade 1C).
We recommend combined pharmacological and IPC thromboprophylaxis within 24 h after bleeding has been controlled and until the patient is mobile (Grade 1B).
We do not recommend the use of graduated compression stockings for thromboprophylaxis (Grade 1C).
We do not recommend the routine use of inferior vena cava filters as thromboprophylaxis (Grade 1C).
IX. Guideline implementation and quality control
Guideline implementation
Recommendation 38
We recommend the local implementation of evidence-based guidelines for management of the bleeding trauma patient (Grade 1B).
Assessment of bleeding control and outcome
Recommendation 39
We recommend that local clinical quality and safety management systems include parameters to assess key measures of bleeding control and outcome (Grade 1B).