CORRESPONDENCE|ONLINE FIRST
Infection rate in Guangzhou after easing the zero-COVID policy: seroprevalence results to ORF8 antigen
Junyuan Huang, Shi Zhao, Ka Chun Chong, et al.
Lancet Infect Dis Published: February 17, 2023
DOI:https://doi.org/10.1016/S1473-3099(23)00112-3
On Dec 7, 2022, the Chinese government announced ten measures indicating the end of the zero-COVID policy, which was in effect for more than 2 years.1 Most of the stringent preventive measures, such as mandatory PCR testing, are no longer required. However, easing of restrictions has contributed to the emergence of new outbreaks predominantly by the SARS-CoV-2 omicron lineages BA5.2 and BF.7 in many cities, such as Beijing.2 With suspension of mass testing in mainland China after adjustment of the zero-COVID policy, empirical data on the epidemic growth and transmissibility of omicron variants are scarce. Until now, the number of infected cases and transmission rates were usually estimated using modelling with partial data.3 Previously, we reported that presence of the ORF8 antibody in blood is one of the most accurate serological markers of SARS-CoV-2 natural infection.4, 5 Because the ORF8 gene is only expressed during SARS-CoV-2 replication, this serology test can confirm whether the patient has previously been infected with the virus and help to estimate the attack ratio.
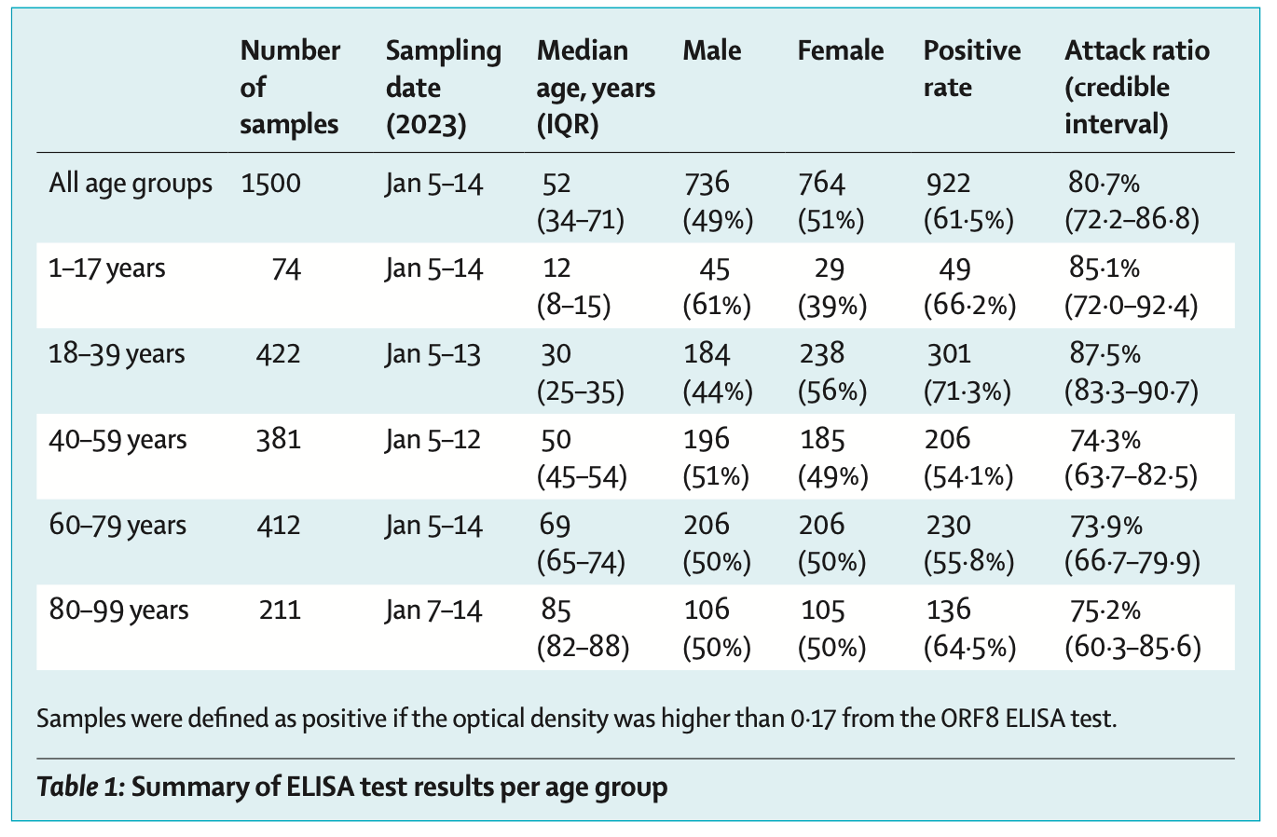
During Jan 5–14, 2023, we collected serum samples from 1500 patients aged 1–99 years at The First Affiliated Hospital of Guangzhou University of Chinese Medicine (Guangzhou, China), around 1 month after the zero-COVID policy was ended. Serum samples were tested using ELISA, with ORF8 protein used as the detection antigen (appendix p 1). The demographic information of patients and ELISA results are shown in the table. The overall positive rate of ORF8 ELISA was 61·5%. The samples were further stratified into five age groups with positive rates of 66·2% in group 1–17 years, 71·3% in group 18–39 years, 54·1% in group 40–59 years, 55·8% in group 60–79 years, and 64·5% in group 80–99 years.
After the zero-COVID policy ended, the age-specific infection attack ratio and disease transmission measures (ie, initial reproduction number and doubling time) were estimated by an age-specific renewal equation. We assumed an initial proportion of susceptibility was 98% on Dec 7, 2022, providing that stringent zero-COVID control measures were implemented in Guangzhou and that there had been no previous large scale COVID-19 outbreaks. The Markov chain Monte Carlo method was used to calculate the posterior estimates and corresponding credible intervals (CIs; appendix).
We estimated that the overall infection attack ratio on the day of the exit strategy was 5·7% (95% CI 4·8–6·8). With an estimated doubling time of 5·3 days (95% CI 4·8–5·8), the overall infection attack ratio rapidly increased to 15·2% (12·3–18·7) at 1 week and 32·9% (26·3–40·2) at 2 weeks after the imposed day of the exit strategy. Among five age groups, individuals aged 1–17 and 18–39 years had higher infection attack ratio than those aged 40–99 years (table; appendix p 1). By day 30 after the exit strategy, the infection attack ratios were 80·7% (95% CI 72·2–86·8) for all age groups, 85·1% (72·0–92·4) for age 1–17 years, 87·5% (83·3–90·7) for age 18–39 years, 74·3% (63·7–82·5) for age 40–59 years, 73·9% (66·7–79·9) for age 60–79 years, and 75·2% (60·3–85·6) for age 80–99 years.
Our research indicates that the COVID-19 epidemic spread fast in mainland China after the zero-COVID control measure was ended. Importantly, these results show that more than 80% of the studied population had already recovered from SARS-CoV-2 omicron infection. Herd immunity to the circulating omicron variants likely is high in Guangzhou and potentially in other urban areas in China with high transmission networks and this wave of transmission in China's urban areas is ceasing.