Intraosseous Abscess from Subacute Osteomyelitis
Haijian Li
N Engl J Med 2026;394:1529
DOI: 10.1056/NEJMicm2514540
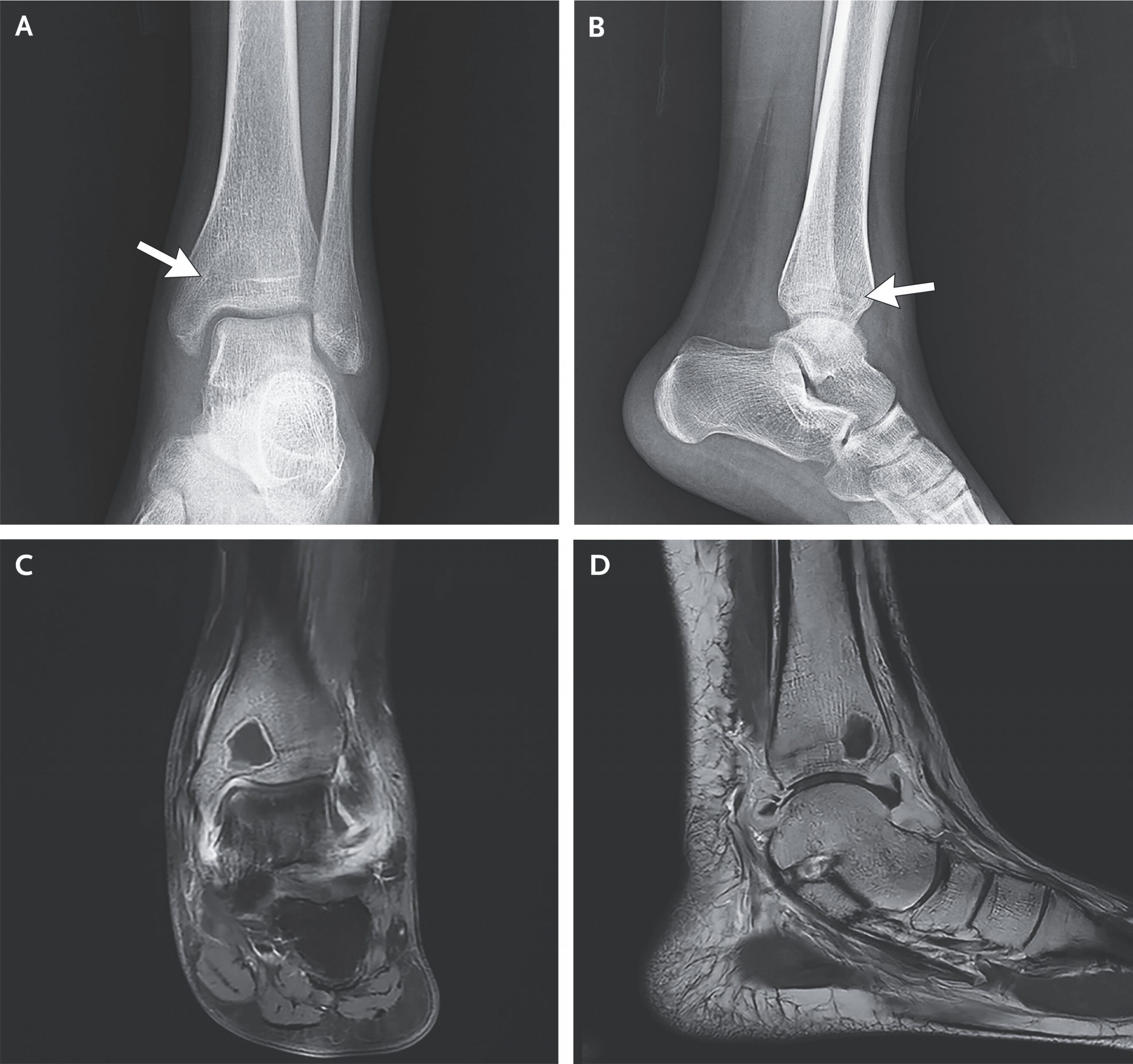
A previously healthy 16-year-old girl presented to the orthopedic clinic with a 1-month history of left ankle pain and an 11-day history of fever. The physical examination was notable for generalized tenderness to palpation of the left ankle, along with a limited active and passive range of motion. Plain radiographs of the ankle (Panel A, anteroposterior view; Panel B, lateral view) showed an ill-defined, radiolucent lesion (arrow) on the distal tibia that crossed the physeal scar (the radio-opaque line at the site of the fused growth plate). There was associated soft-tissue swelling but no fracture or periosteal reaction. Owing to concern about an aggressive infection or neoplasm, magnetic resonance imaging (MRI) of the leg was performed. The images showed a lesion measuring 14 mm by 16 mm by 12 mm on the distal tibia (Panel C, coronal view; Panel D, sagittal view); the lesion was hypointense and surrounded by a hyperintense sclerotic rim, a finding known as the penumbra sign, which is specific for subacute osteomyelitis. A diagnosis of an intraosseous abscess — also known as a Brodie’s abscess — from subacute osteomyelitis was made. The patient was treated with surgical débridement and a course of antibiotic agents. Metagenomic sequencing of the débrided tissue identified Salmonella enterica. At 3 months after completion of the course of antibiotics, the patient’s symptoms had completely resolved.