ARTICLES March 21, 2026Open Access
Endotracheal surfactant for infants with life-threatening bronchiolitis (BESS): a randomised, blinded, sham-controlled, phase 2 trial
Malcolm G Semple, Chloe Donohue, Laura Price, et al
Lancet Respir Med Published March 21, 2026
DOI: 10.1016/S2213-2600(26)00008-1
Summary
Background
Bronchiolitis is a common viral respiratory disease of infants, with severity ranging from mild symptoms, such as coryza and feeding difficulties, to fulminant respiratory failure. Endotracheal administration of exogenous surfactant has been shown in small studies to improve gas exchange in critically ill infants with bronchiolitis. We aimed to investigate the safety and efficacy of endotracheal poractant alfa for treating critical bronchiolitis compared with a sham procedure.
Methods
BESS was a multicentre, blinded, randomised, sham-controlled, parallel-group, phase 2, superiority trial with exploratory mechanism evaluation studies. The trial was done in 15 paediatric intensive care units in the devolved National Health Service (NHS) of England, Scotland, and Northern Ireland. Preterm and term-born infants younger than 26 weeks of gestationally corrected age admitted to hospitals with bronchiolitis requiring invasive mechanical ventilation (IMV) were randomly assigned (1:1) to receive up to three doses of endotracheal poractant alfa (Curosurf) or sham intervention, allocated through web-based randomisation. Randomisation was stratified by duration of IMV before randomisation (<24 h and ≥24 h) and by site. The infants and their families, clinical care staff, Liverpool Clinical Trial Centre staff, and members of the site research teams were masked to treatment allocations. Endotracheal poractant alfa was given initially at 200 mg/kg, followed by 100 mg/kg at 12 h intervals. The primary endpoint was the duration of IMV from randomisation to final successful extubation. All infants who were successfully extubated were included in the intention-to-treat analysis. Safety outcomes were analysed in infants who had received at least one trial intervention. This trial was registered prospectively with ISRCTN (ISRCTN11746266) and EudraCT (2018–001169–18), and is completed.
Findings
The trial was completed after six recruitment seasons. Between Dec 18, 2018, to March 31, 2024, 1009 infants were assessed for eligibility, 232 of whom were randomly assigned to receive either endotracheal poractant alfa (n=115) or a sham intervention (n=117). 130 (56%) of 232 infants were male and 102 (44%) were female. Three infants were withdrawn from the study. None were lost to follow-up. The median duration of IMV was 64·9 h (IQR 43·2–92·1) in the endotracheal poractant alfa group and 62·0 h (39·3–95·1) in the sham intervention group. The geometric mean ratio was 1·02 (95% CI 0·84–1·24; t-test p=0·86). No clinically significant safety issues were associated with endotracheal poractant alfa and there were no deaths.
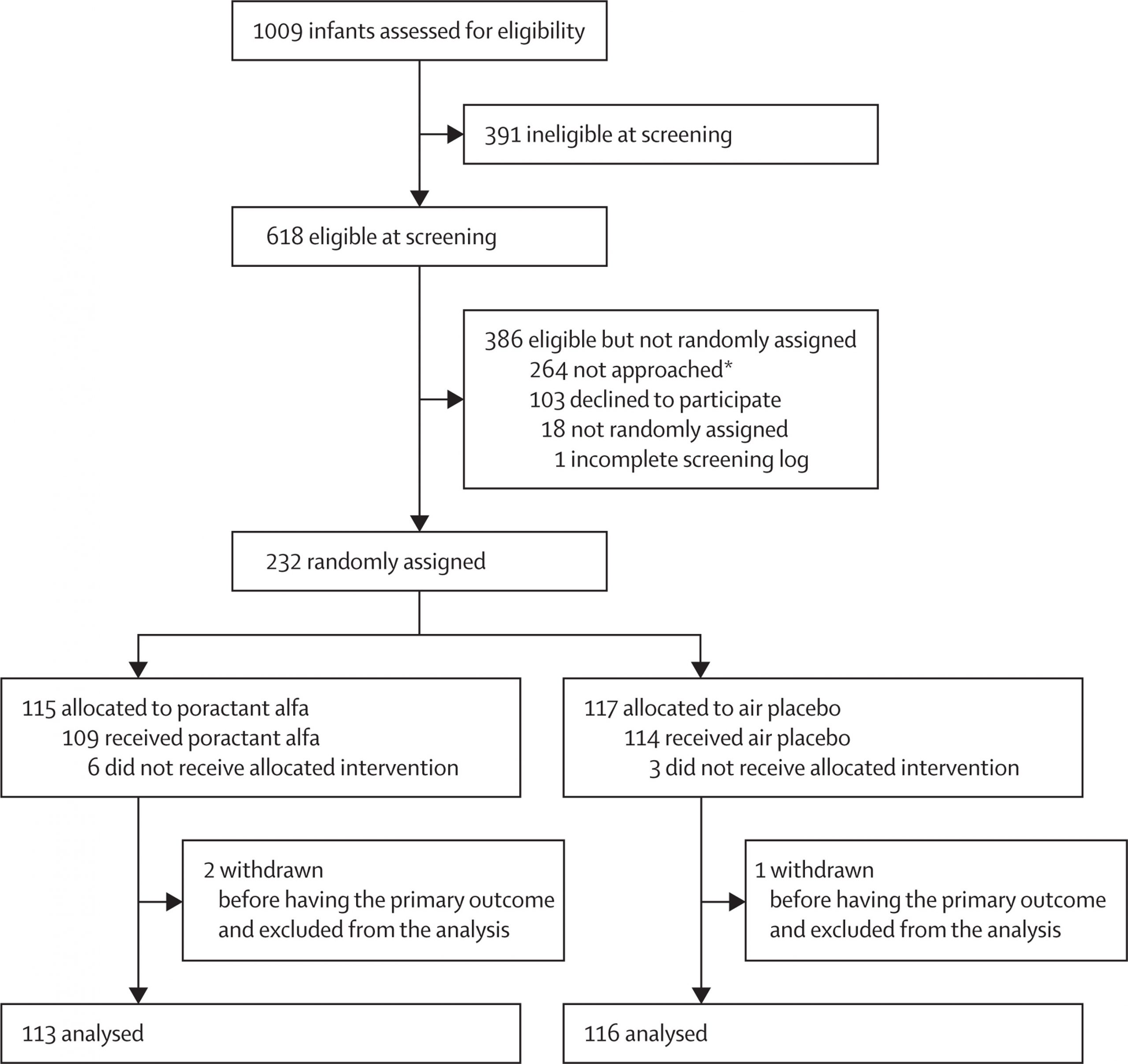
Table 1Baseline demographic and clinical characteristics at randomisation
| Endotracheal poractant alfa group (n=115) | Sham intervention group (n=117) | ||
|---|---|---|---|
| Sex | |||
| Male | 63 (55%) | 67 (57%) | |
| Female | 52 (45%) | 50 (43%) | |
| Premature birth | |||
| Yes | 66 (57%) | 61 (52%) | |
| No | 49 (43%) | 56 (48%) | |
| Gestational age | |||
| Extremely preterm (<28 weeks) | 5 (4%) | 5 (4%) | |
| Very preterm (28–31 weeks) | 7 (6%) | 13 (11%) | |
| Moderate preterm (32–33 weeks) | 11 (10%) | 12 (10%) | |
| Late preterm (34–39 weeks) | 39 (34%) | 27 (23%) | |
| Term (≥40 weeks) | 49 (43%) | 56 (48%) | |
| Not known | 4 (3%) | 4 (3%) | |
| Gestational age, weeks* | |||
| Mean | 36·7 (3·9) | 36·5 (4·4) | |
| Median | 38·0 (34·0 to 40·0) | 39·0 (33·0 to 40·0) | |
| Range | 26·0 to 40·0 | 24·0 to 40·0 | |
| Age corrected for gestation at randomisation, all infants, weeks | |||
| Mean | 5·0 (6·5) | 4·8 (5·9) | |
| Median | 4·0 (0·0 to 8·0) | 3·0 (1·0 to 7·0) | |
| Range | −5·0 to 25·0 | −4·0 to 23·0 | |
| Median age of premature born infants at randomisation, corrected for gestation, weeks | n=66; 1·0 (−1·0 to 5·0) | n=61; 2·0 (−1·0 to 4·0) | |
| Median age of term-born infants at randomisation, weeks† | n=49; 6·0 (4·0 to 11·0) | n=56; 6·0 (3·0 to 10·0) | |
| Weight, all infants, kg | |||
| Mean | 4·2 (1·5) | 4·2 (1·5) | |
| Median | 4·0 (3·0 to 5·0) | 4·0 (3·1 to 5·0) | |
| Range | 2·0 to 8·9 | 2·0 to 8·8 | |
| Intubated on arrival to the PICU | |||
| Yes | 90 (78%) | 97 (83%) | |
| No | 25 (22%) | 20 (17%) | |
| Median time on mechanical ventilator before arrival at PICU, h | 30·1 (22·7 to 37·0) | 29·9 (21·3 to 37·1) | |
| Data unobtainable | 4 (3%) | 1 (1%) | |
| Bacterial infection identified | |||
| Yes | 29 (25%) | 31 (26%) | |
| No | 79 (69%) | 82 (70%) | |
| No sample taken | 4 (3%) | 2 (2%) | |
| Data unobtainable | 3 (3%) | 2 (2%) | |
| Viral infection identified | |||
| Yes | 101 (88%) | 111 (95%) | |
| No | 8 (7%) | 5 (4%) | |
| No sample taken | 4 (3%) | 0 | |
| Data unobtainable | 2 (2%) | 1 (1%) | |
* Data on gestational age were only collected for those infants who were deemed to be preterm.
† Negative value indicates a negative corrected age.
Table 2Primary and secondary continuous outcome results
| Endotracheal poractant alfa group* (n=115) | Sham intervention group* (n=117) | Geometric mean ratio (95% CI) | p value | |
|---|---|---|---|---|
| Total duration of mechanical ventilation, h | 64·9 (43·2–92·1) | 62·0 (39·3–95·1) | 1·02 (0·84 to 1·24) | 0·86 |
| Time to readiness for spontaneous breathing trial, h | 57·3 (32·4–75·6) | 37·2 (25·6–81·4) | 0·99 (0·75–1·31) | 0·94 |
| Duration of oxygen supplementation, h | 40·9 (17·0–90·0) | 34·0 (16·0–81·4) | 2·42 (1·03–5·68) | 0·043 |
| Duration of post-extubation respiratory support, h | 0·0 (0·0–15·7) | 0·0 (0·0–0·0) | 1·68 (0·48–5·80) | 0·41 |
| Duration of stay at PICU, h | 104·4 (67·9–153·1) | 93·4 (66·6–144·8) | 1·01 (0·86–1·18) | 0·95 |
| Duration of total stay in hospital, h | 165·3 (111·3–231·2) | 142·2 (96·6–221·9) | 1·13 (0·96–1·33) | 0·13 |
* Data are median (IQR) of the raw data with no transformations in hours.
Table 3Non-serious adverse events
| Endotracheal poractant alfa group | Sham intervention group | ||||
|---|---|---|---|---|---|
| Events | Patients (n=109) | Events | Patients (n=114) | ||
| Total | 17 | 14 (13%) | 9 | 8 (7%) | |
| Cardiac disorders: bradycardia | 4 | 4 (4%) | 0 | 0 | |
| Ear and labyrinth disorders: otorrhoea | 0 | 0 | 1 | 1 (1%) | |
| General disorders and administration site conditions | |||||
| Perforation | 0 | 0 | 1 | 1 (1%) | |
| Pyrexia | 0 | 0 | 1 | 1 (1%) | |
| Total | 0 | 0 | 2 | 2 (2%) | |
| Infections and infestations | |||||
| Bronchiolitis* | 0 | 0 | 1 | 1 (1%) | |
| Pneumonia | 1 | 1 (1%) | 0 | 0 | |
| Total | 1 | 1 (1%) | 1 | 1 (1%) | |
| Injury, poisoning, and procedural complications | |||||
| Endotracheal intubation complication | 1 | 1 (1%) | 1 | 1 (1%) | |
| Sedation complication | 1 | 1 (1%) | 0 | 0 | |
| Total | 2 | 2 (2%) | 1 | 1 (1%) | |
| Investigations: oxygen saturation decreased | 5 | 4 (4%) | 0 | 0 | |
| Metabolism and nutrition disorders | |||||
| Hypokalaemia | 1 | 1 (1%) | 0 | 0 | |
| Total | 1 | 1 (1%) | 0 | 0 | |
| Nervous system disorders: epilepsy | 0 | 0 | 1 | 1 (1%) | |
| Reproductive system and breast disorders: genital discharge | 1 | 1 (1%) | 0 | 0 | |
| Respiratory, thoracic and mediastinal disorders | |||||
| Atelectasis | 0 | 0 | 1 | 1 (1%) | |
| Hypoxia | 0 | 0 | 1 | 1 (1%) | |
| Respiratory depth decreased | 1 | 1 (1%) | 0 | 0 | |
| Total | 1 | 1 (1%) | 2 | 2 (2%) | |
| Extubation | 2 | 2 (2%) | 1 | 1 (1%) | |
Interpretation
Poractant alfa, administered endotracheally to infants with early critical bronchiolitis, although safe, did not reduce the duration of IMV compared with the sham intervention. Therefore, our findings suggest that it should not be used for this indication at this dose and administration method.
Funding
UK National Institute for Health and Care Research, UK Research and Innovation Medical Research Council, Chief Scientist Office Scotland, Health and Social Care Research and Development Division Northern Ireland, and Chiesi Farmaceutici, Italy.