Massive Intravascular Hemolysis from Clostridium perfringens Bacteremia
Ann Tran, Carol Lee
N Engl J Med 2026;394: e19
DOI: 10.1056/NEJMicm2514135
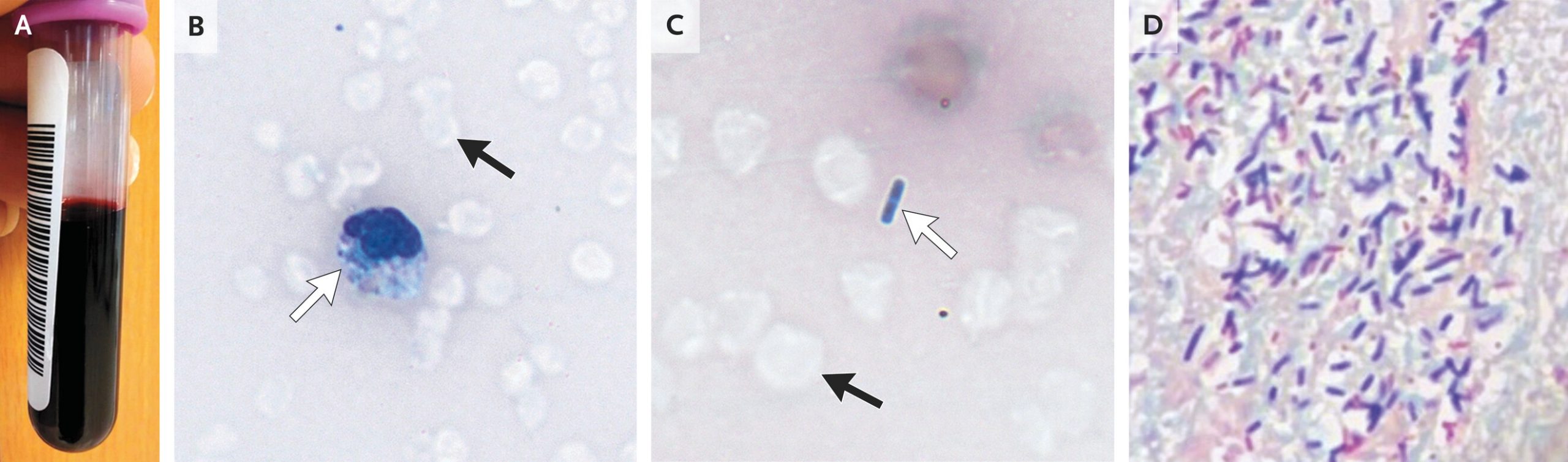
A 73-year-old woman with type 2 diabetes presented to the emergency department with a 1-day history of malaise, dyspnea, and confusion. Vital signs and physical examination indicated shock. Serum laboratory samples were obtained, but they could not be processed owing to gross hemolysis. Even after centrifugation, the specimen resembled whole blood (Panel A). Approximately 45 minutes after arrival, the patient had a pulseless electrical activity cardiac arrest and died despite attempted cardiopulmonary resuscitation. A postmortem review of a peripheral-blood smear showed numerous dehemoglobinized red cells (Panels B and C, black arrows; Wright–Giemsa stain) with intracellular (Panel B, white arrow) and extracellular (Panel C, white arrow) bacilli. On autopsy, cardiac tissue showed numerous gram-positive and gram-negative bacilli, with gram-positive organisms predominating (Panel D, Gram’s stain). Postmortem blood cultures grew Clostridium perfringens and Klebsiella pneumoniae. A diagnosis of massive intravascular hemolysis from C. perfringens bacteremia was made. This condition results from bacterial toxin release and is associated with very high mortality. Although the diagnosis is rare, clinicians may consider this type of in vivo hemolysis when treating patients with undifferentiated illness who are in shock and whose blood samples are grossly hemolyzed. Although a gastrointestinal source of polymicrobial bacteremia was suspected in this case, the definitive cause was not identified on autopsy.