Article
Hemodynamic and neurological presentations of invasive meningococcal disease in adults: a nationwide study across 100+ French ICUs: The RETRO-MENINGO study
Damien Contou, Benoit Painvin, Delphine Daubin, et al
Intensive Care Med 2025; 51: 1587-1602
Abstract
Purpose
Invasive meningococcal disease (IMD) is a rare but potentially fatal infection caused by Neisseria meningitidis. In adults requiring admission to intensive care unit (ICU), IMD typically presents with two distinct clinical presentations: neurological (meningitis) and hemodynamic (sepsis). These presentations are often conflated, despite the differences in pathophysiology and outcome.
Methods
RETRO-MENINGO is a nationwide, multicentre, retrospective cohort study conducted in 102 French ICUs between January 1, 2016, and December 31, 2024. Adults (≥ 18 years) admitted to the ICU with a microbiologically confirmed IMD were categorised as having either a neurological or a hemodynamic presentation according to the main reason for ICU admission. The primary outcome was day-60 mortality in each presentation.
Results
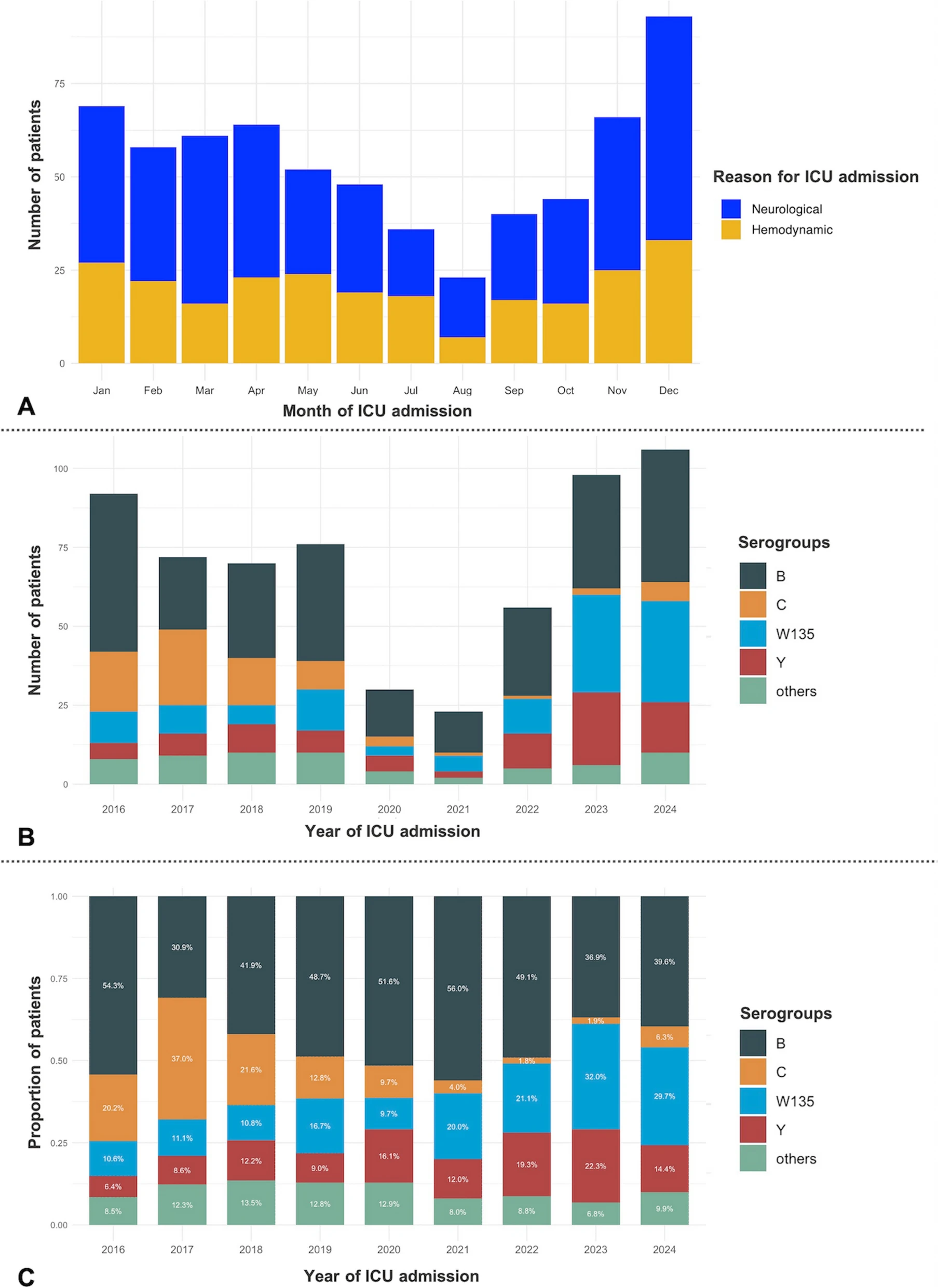
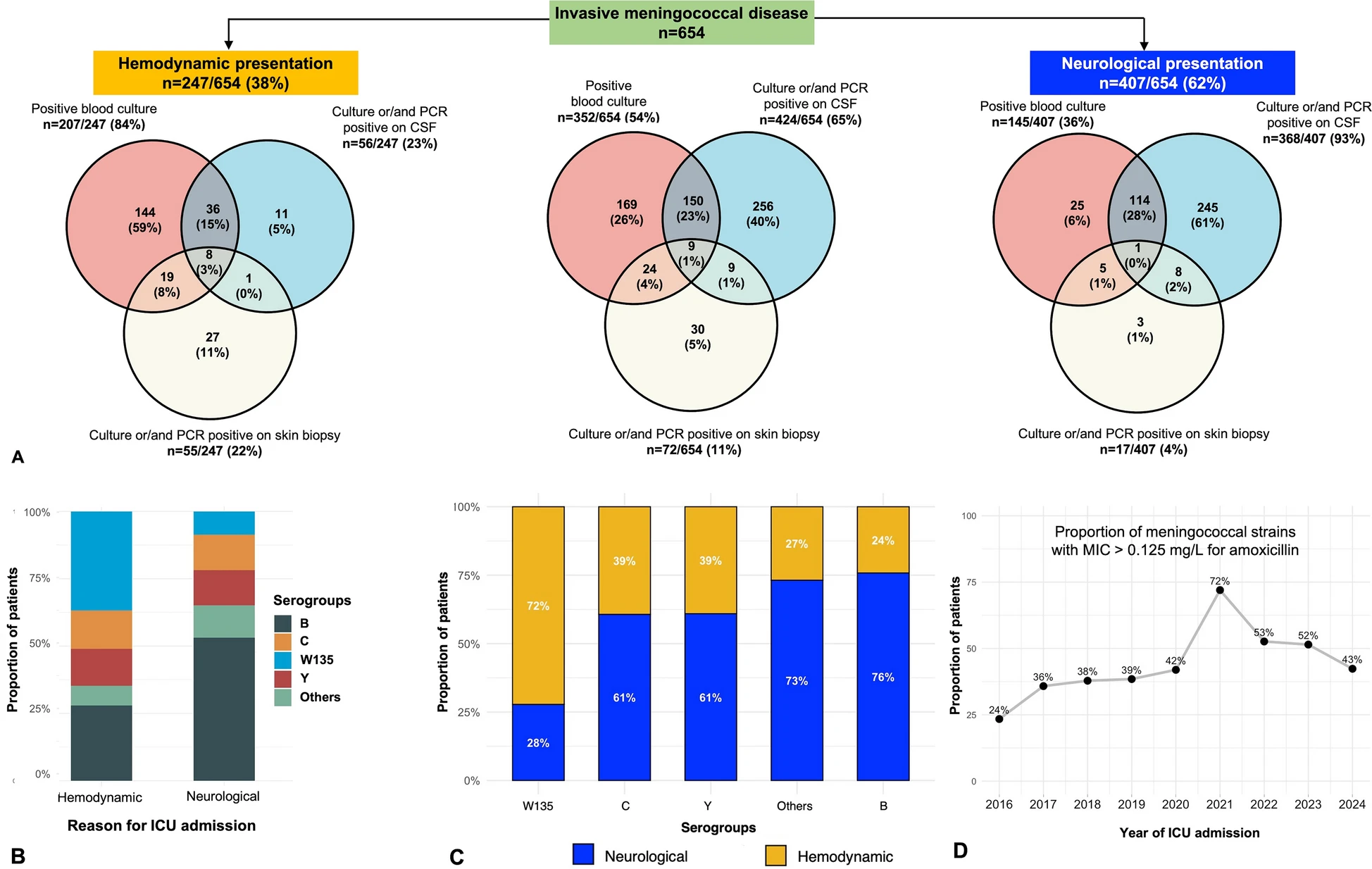
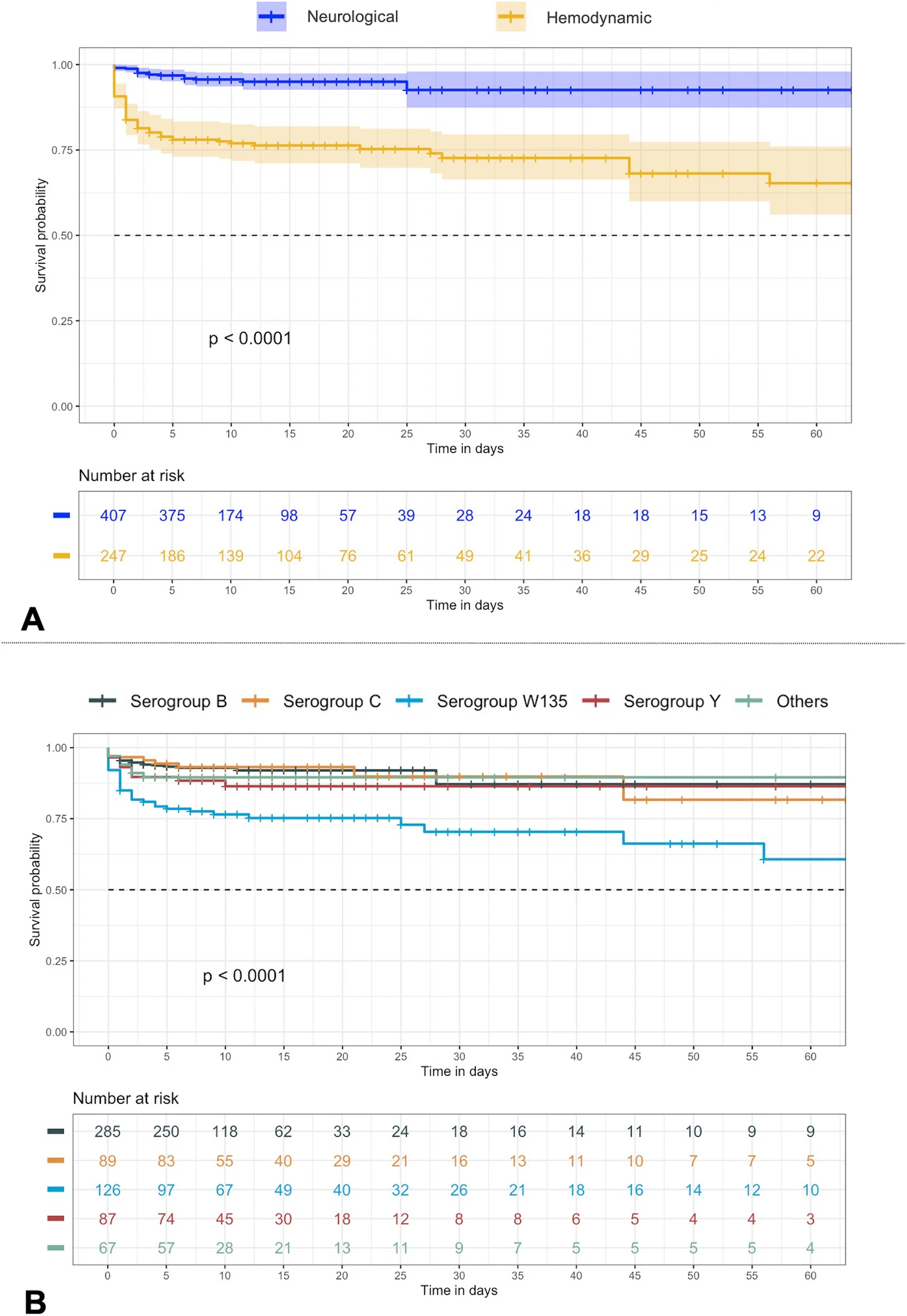
Of 654 patients (median age 33 years [IQR 21–56]; 63.5% without comorbidities), 407 (62%) had a neurological and 247 (38%) a hemodynamic presentation at ICU admission. Hemodynamic presentation was associated with older age (39.0 vs. 30.0 years; p = 0.001), immunosuppression (17.0% vs. 7.1%; p < 0.001), purpuric rash (55.9% vs. 43.7%; p = 0.003), earlier ICU admission (1 vs. 2 days; p = 0.001) and more frequent bacteremia (83.8% vs. 35.6%; p < 0.001). Serogroup B was predominant in neurological presentation, whereas serogroup W135 was more common in hemodynamic presentation. Compared to neurological presentation, hemodynamic presentation required more organ support (vasopressors, invasive mechanical ventilation, transfusions, renal replacement therapy) and had a significantly higher day-60 mortality (25.5% vs. 4.7%; p < 0.001). Hemodynamic presentation (aOR 4.33, 95% CI 2.26–8.62; p < 0.001), absence of comorbidities (aOR 2.21, 95% CI 1.19–4.23; p = 0.014), age > 35 years (aOR 3.65, 95% CI 1.73–6.07; p < 0.001), arterial lactate level > 5 mmol/L (aOR 2.60, 95% CI 1.43–4.77; p = 0.002) and symptom onset < 24 h (aOR 1.90, 95% CI 1.00–3.55; p = 0.040) were independently associated with day-60 mortality, while early administration of a parenteral third-generation cephalosporin prior to ICU admission was strongly protective (aOR 0.31, 95% CI 0.18–0.55; p < 0.001).

Conclusion
Neurological and hemodynamic presentation of IMD are clinically and prognostically distinct. Recognition of these phenotypes is critical for appropriate management and prediction of outcome.