Transfusion strategies in bleeding critically ill adults: a clinical practice guideline from the European Society of Intensive Care Medicine
Alexander P. J. Vlaar, Joanna C. Dionne, Sanne de Bruin, et al
Intensive Care Medicine 2021; 47: 1368-1392
Transfusion support in massively bleeding, critically ill adults
Part 1: massively bleeding patients
1. Transfusion ratios
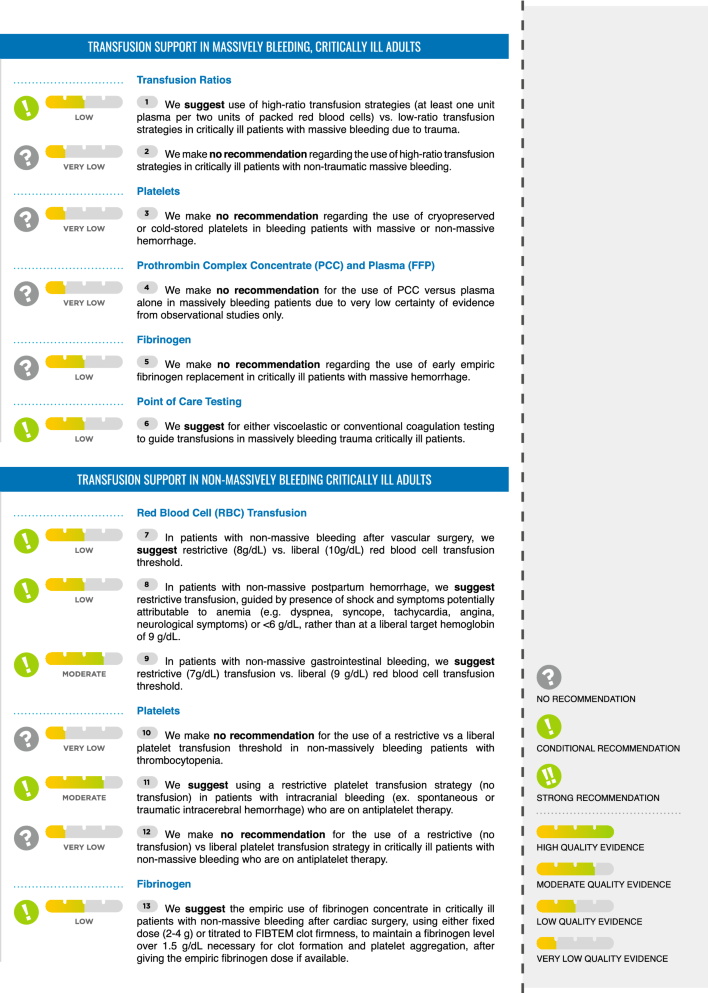
We suggest use of high-ratio transfusion strategies (at least one unit plasma per two units of packed red blood cells) vs. low-ratio transfusion strategies in critically ill patients with massive bleeding due to trauma (Conditional recommendation, low certainty of evidence).
We make no recommendation regarding the use of fixed high-ratio transfusion strategies in critically ill patients with non-traumatic massive bleeding (No recommendation, very low certainty evidence).
2. Platelets
We make no recommendation regarding the use of cryopreserved or cold-stored platelets in bleeding patients with massive or non-massive hemorrhage (No recommendation, very low certainty of evidence).
3. Prothrombin complex concentrate (PCC) and plasma
We make no recommendation for the use of PCC versus plasma alone in massively bleeding patients due to very low certainty of evidence from observational studies only (No recommendation, very low certainty of evidence)
4. Fibrinogen
We make no recommendation regarding the use of early empiric fibrinogen replacement in critically ill patients with massive hemorrhage due to trauma (No recommendation, low certainty evidence).
5. Point of care testing
We suggest for either for viscoelastic or conventional coagulation assays to guide transfusions in massively bleeding trauma critically ill patients (Conditional recommendation, low quality of evidence)
Part 2: transfusion support in non‑massively bleeding critically ill adults
1. RBC transfusion
In patients with non-massive bleeding after vascular surgery, we suggest restrictive (7.5–8 g/ d/L) red blood cell transfusion threshold (Conditional recommendation, low certainty).
In patients with non-massive postpartum hemorrhage, we suggest restrictive transfusion, guided by presence of shock and symptoms potentially attributable to anemia (e.g. dyspnea, syncope, tachycardia, angina, neurological symptoms) or hemoglobin < 6 g/dL, rather than at a liberal target hemoglobin of 9 g/dL (Conditional recommendation, low certainty).
In patients with non-massive gastrointestinal bleeding, we suggest restrictive (7 g/dL) transfusion vs. liberal (9 g/dL) red blood cell transfusion threshold (Conditional recommendation, moderate certainty).
2. Platelets
We make no recommendation for the use of a restrictive vs a liberal platelet transfusion threshold in non-massively bleeding patients with thrombocytopenia (No recommendation, very low certainty evidence)
We suggest using a restrictive platelet transfusion strategy (no transfusion) in patients with intracranial hemorrhage (spontaneous or traumatic intracerebral hemorrhage) who are on antiplatelet therapy (Conditional recommendation, moderate certainty evidence).
We make no recommendation for the use of a restrictive (no transfusion) vs liberal platelet transfusion strategy in critically ill patients with non-massive bleeding who are on antiplatelet therapy (No recommendation, very low certainty of evidence)
3. Fibrinogen
We suggest the empiric use of fibrinogen concentrate in critically ill patients with non-massive bleeding after cardiac surgery, using either fixed dose (2–4 g) or titrated to FIBTEM clot firmness, to maintain a fibrinogen level over 1.5 g/dL necessary for clot formation and platelet aggregation, after giving the empiric fibrinogen dose if available (Conditional recommendation, low certainty of evidence).
We make no recommendation regarding the empiric use of fibrinogen concentrate in other critically ill patients with non-massive bleeding (No recommendation, low certainty of evidence)
4. Plasma
We make no recommendation for a restrictive plasma versus a liberal plasma transfusion strategy for non-massively bleeding patients with or without coagulopathy (No recommendation, low certainty evidence)
5. Point of care vs. conventional coagulation testing
We suggest either viscoelastic testing or conventional coagulation testing to guide transfusions in massive and non-massively bleeding cirrhotic patients, liver transplant patients or critically ill trauma patients (Conditional recommendation, low certainty evidence).
We suggest either viscoelastic testing or conventional coagulation testing to guide transfusions in bleeding cardiac surgery patients (Conditional recommendation, very low certainty of evidence).
We suggest using either viscoelastic testing or conventional coagulation testing to guide transfusion in extra corporeal membrane oxygenation (ECMO) patients with non-massive bleeding (Conditional recommendation, very low certainty evidence).
Part 3. Tranexamic acid (TXA) in bleeding critically ill adults
1. TXA in patients with traumatic intracranial hemorrhage
We recommend the use of early (< 3 h from trauma) TXA in critically ill patients with bleeding or suspected bleeding due to trauma (Strong recommendation, high certainty).
We suggest the use of TXA in critically ill patients with acute traumatic brain injury and bleeding due to trauma (Conditional recommendation, moderate certainty).
We make no recommendation regarding the use of TXA in critically ill patients with subarachnoid hemorrhage (No recommendation, low certainty evidence).
2. TXA in patients with non‑traumatic intracranial hemorrhage.
We make no recommendation regarding the use of TXA in critically ill patients non-traumatic intracranial hemorrhage (No recommendation, moderate certainty).
We suggest not using high-dose IV TXA in critically ill patients with gastrointestinal bleeding (Conditional recommendation, high certainty evidence).
We make no recommendation regarding the use of low-dose IV TXA or enteral TXA in critically ill patients with gastrointestinal bleeding (No recommendation, moderate certainty evidence)
We suggest the early use of TXA in critically ill patients with postpartum hemorrhage (Conditional recommendation, high certainty).
We recommend the use of TXA in critically ill patients with bleeding post-cardiac surgery (Strong recommendation, high certainty).