PERIOPERATIVE MEDICINE
Individualized Flow-controlled versus Pressure-controlled Ventilation in Cardiac Surgery: A Randomized Controlled Trial
Becker, Simon; Kurz, Christian T; Schnitzler, Romina, et al
Anesthesiology January 14, 2026. | DOI: 10.1097/ALN.0000000000005851
Background:
Patients undergoing on-pump cardiac surgery are at high risk for perioperative lung injury and a hyperinflammatory state associated with postoperative complications. The authors investigated the hypothesis that flow-controlled ventilation (FCV) reduces the inflammatory stimulus compared to conventional pressure-controlled ventilation (PCV) in this patient cohort. FCV has the unique feature of controlling airway flows during inspiration and expiration and the potential to reduce mechanical power of invasive ventilation.
Methods:
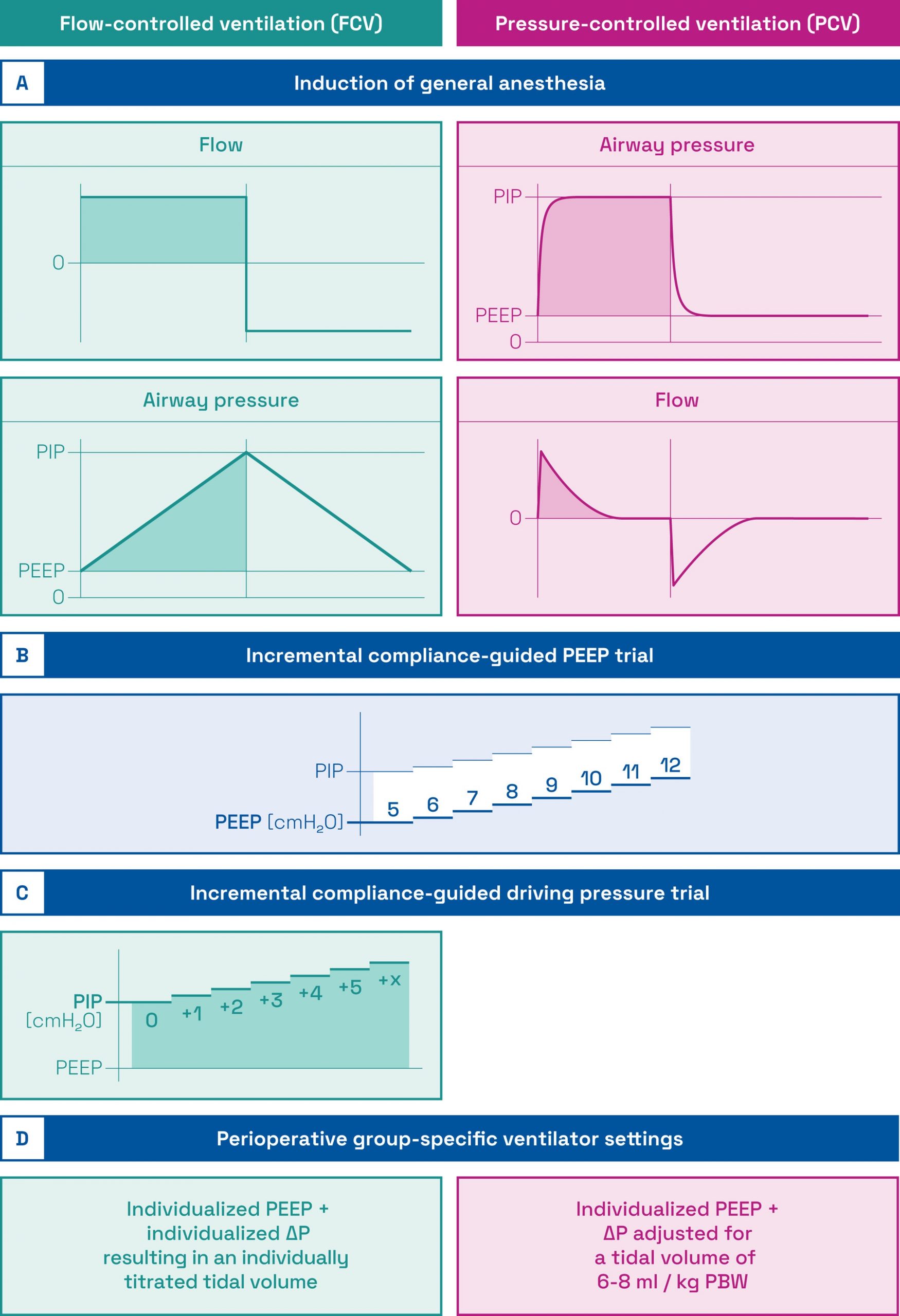
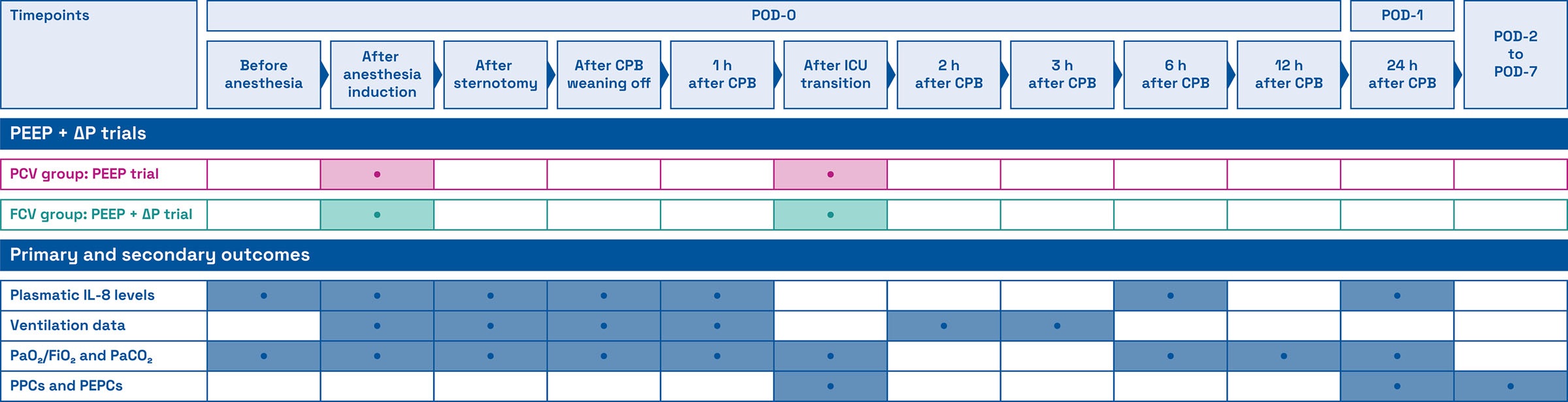
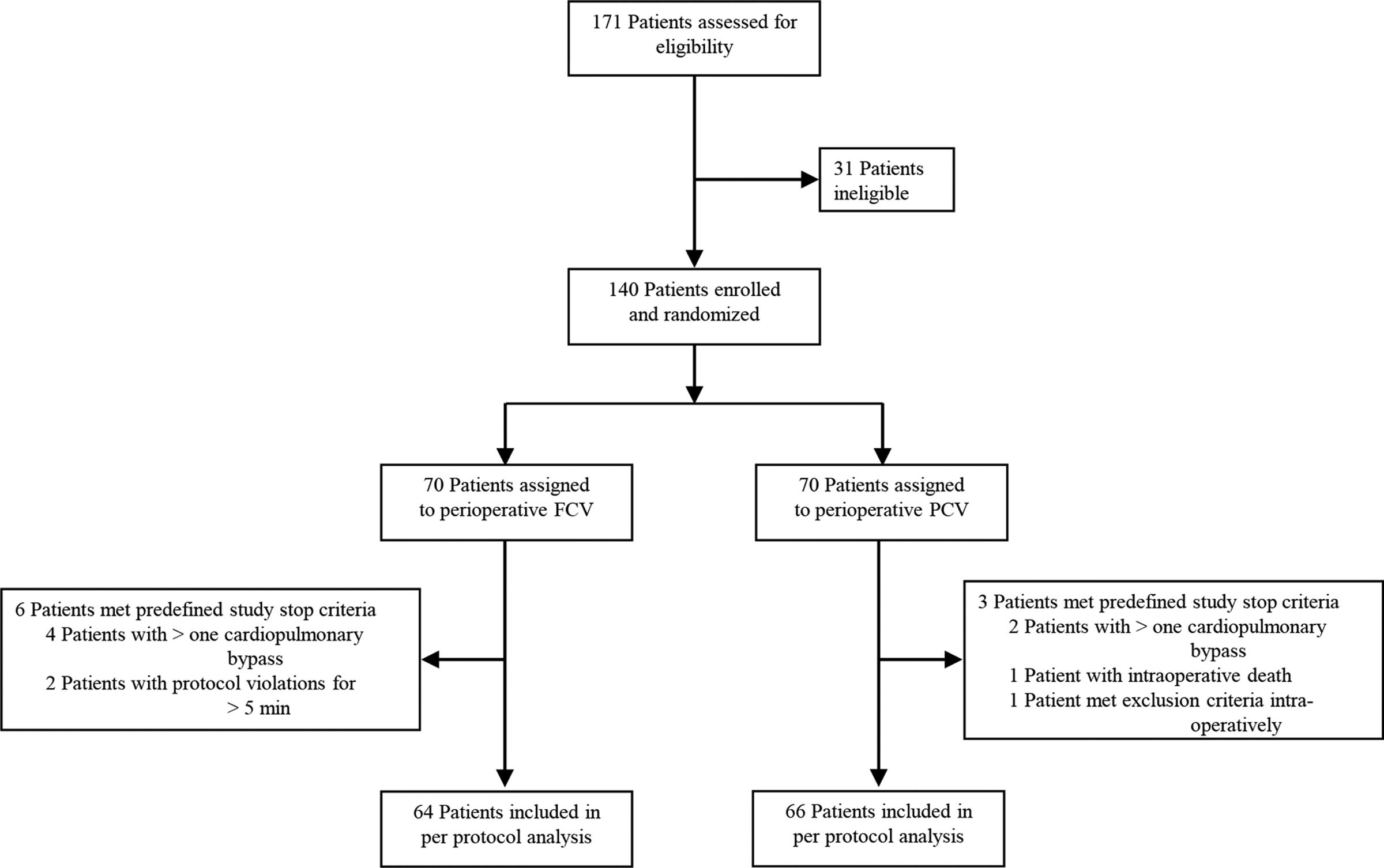
In this single-center randomized controlled trial, 140 adult patients undergoing cardiac surgery with cardiopulmonary bypass were allocated 1:1 to FCV or PCV from August 10, 2020, to November 16, 2022. Participants received perioperatively either individualized FCV with a compliance-guided positive end-expiratory pressure (PEEP) and a compliance-guided driving pressure (ΔP) or PCV with a compliance-guided PEEP and ΔP for tidal volumes of 6 to 8 ml/kg predicted body weight. Postoperative plasmatic interleukin 8 (IL-8) levels 6 h after cardiopulmonary bypass were defined as the primary endpoint. Explorative secondary outcomes included incidences of postoperative pulmonary and extrapulmonary complications and hospital length of stay.
Results:
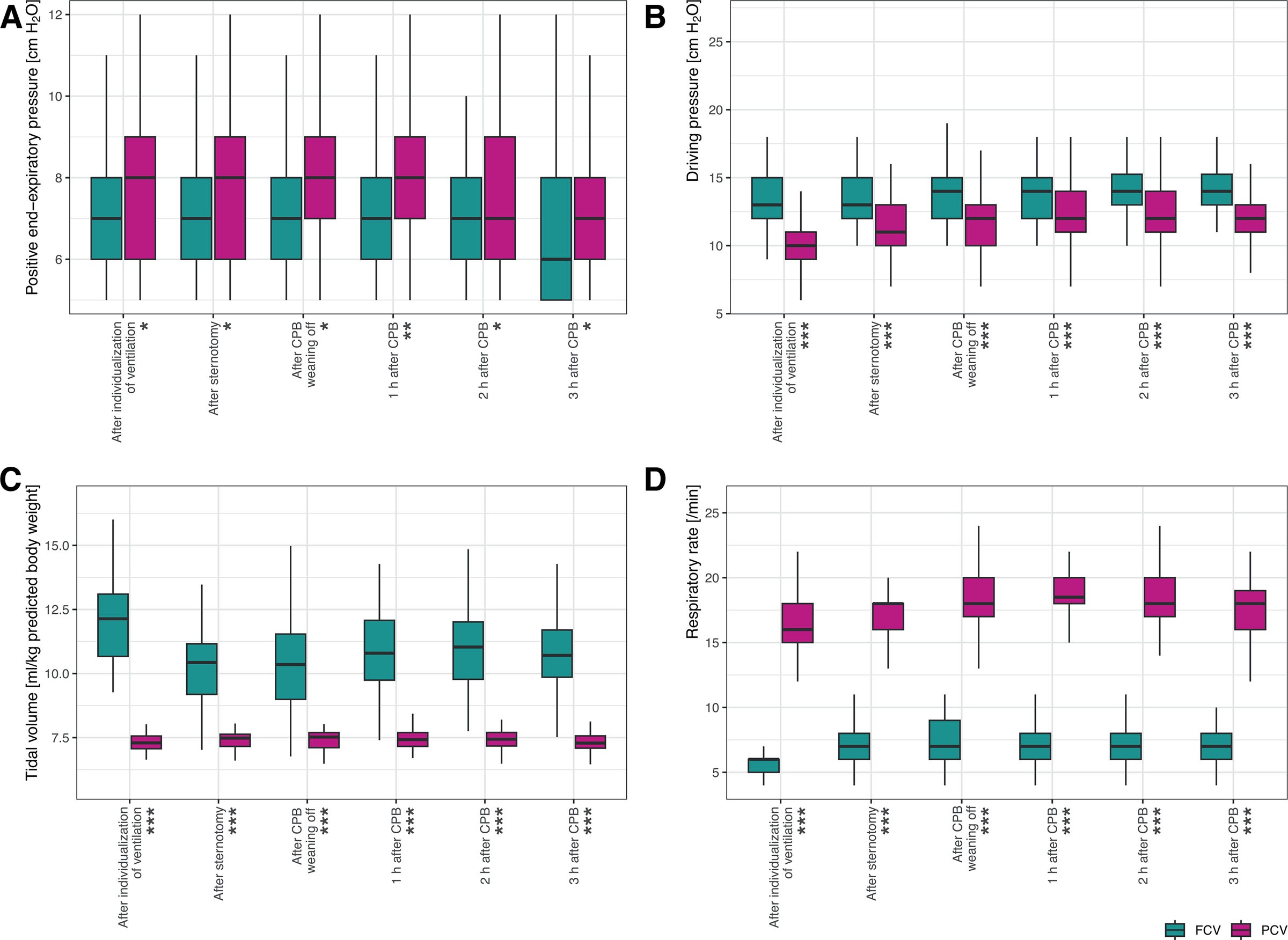
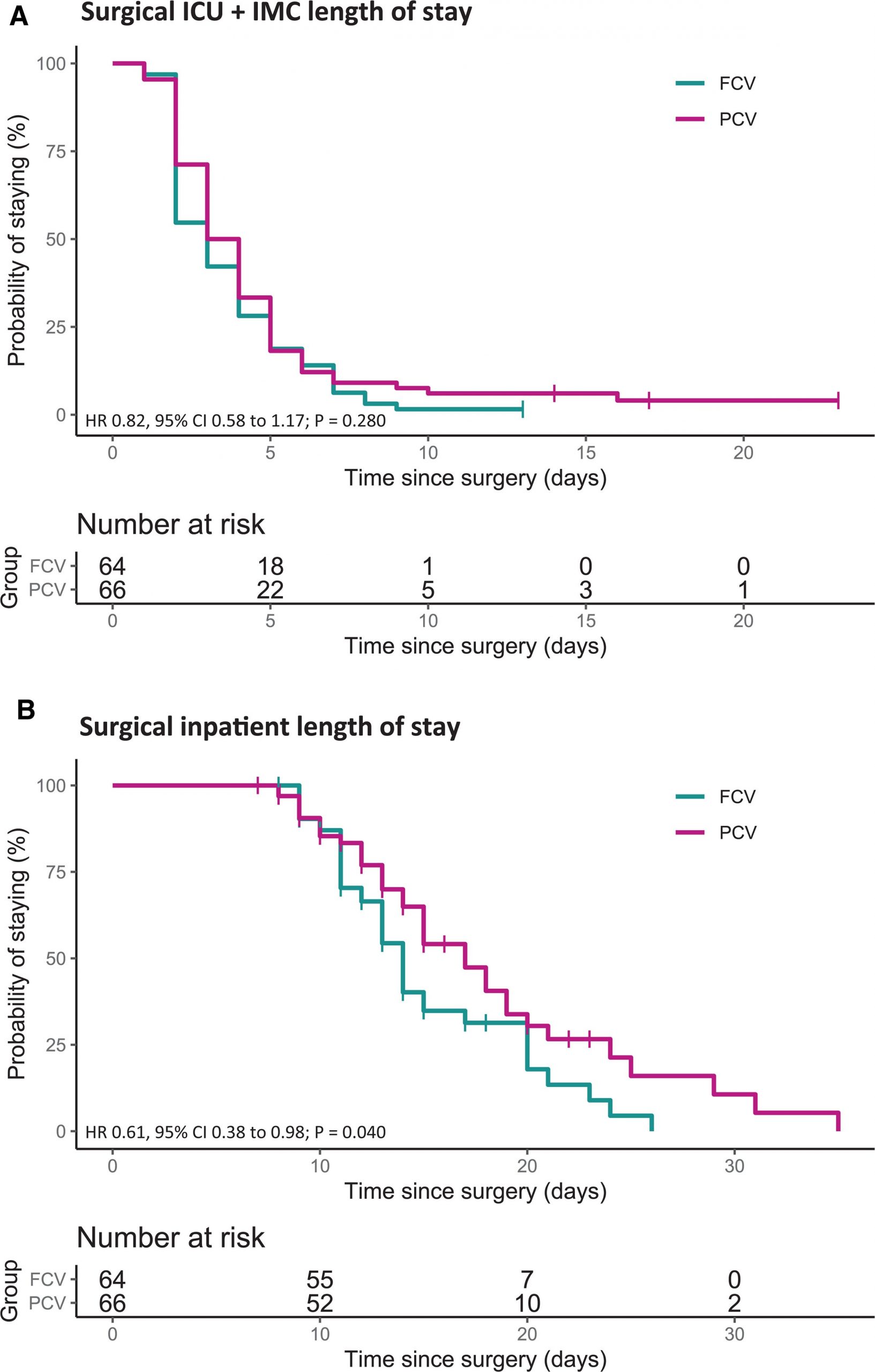
Median postoperative IL-8 levels did not differ significantly between FCV and PCV (FCV, 3.08 vs. PCV, 3.60; β, 0.08 pg/ml; 95% CI, −0.17 to 0.33; P = 0.573). ΔP values and tidal volumes were higher in the FCV group but FCV yielded lower respiratory rates and minute volumes required for normocapnia. As a result, the FCV approach reduced the perioperatively applied mechanical power by 55%. After FCV, incidences of single postoperative pulmonary complications (e.g., confirmed pneumonia, moderate and severe hypoxemia) and any postoperative extrapulmonary complication were lower and the hospital stay shorter.
Conclusions:
FCV did not reduce plasmatic IL-8 levels at the predefined timepoint 6 h after cardiopulmonary bypass. However, the reduction of mechanical power during individualized FCV application and the findings of the explorative secondary study outcomes justify future trials.