Imaging in Intensive Care Medicine
Ghost cells in Clostridium perfringens liver abscess with massive hemolysis
Yoshihiro Nagai, Seiya Nishiyama, Tadashi Kamio, et al
Intensive Care Med 2025
https://doi.org/10.1007/s00134-025-08227-y
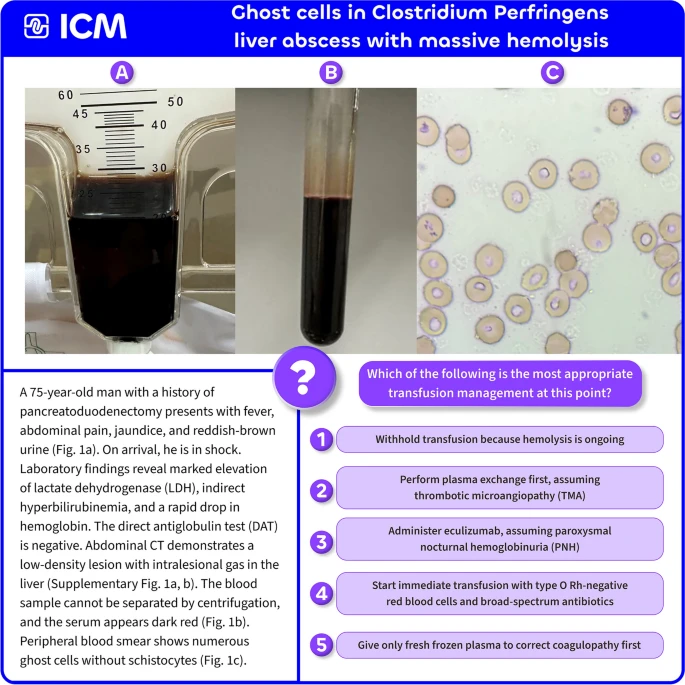
Clostridium perfringens produces phospholipase C, the systemic dissemination of which can lead to severe intravascular hemolysis. Erythrocytes whose cell membranes are lysed lose hemoglobin, and the resulting small, membrane-only remnants are observed as ghost cells. Conversely, the presence of schistocytes is reportedly rare, which represents a major distinguishing feature from thrombotic microangiopathy (TMA). In patients presenting with suspected severe infection, such as in this case, the combination of severe intravascular hemolysis that prevents blood centrifugation and the observation of ghost cells on peripheral blood smear should prompt the immediate consideration of Clostridium perfringens as the causative organism.
This image (Figure 1) is highly suggestive of Clostridium perfringens sepsis with fulminant intravascular hemolysis. Because the circulating hemoglobin no longer reflects the actual oxygen-carrying capacity, withholding transfusion is life-threatening. Immediate transfusion with uncrossmatched type O Rh-negative red blood cells should be initiated, together with high-dose penicillin and clindamycin to suppress toxin production. Simultaneous source control (e.g., drainage of hepatic abscess) is essential. Although transfused RBCs may undergo further hemolysis, maintaining tissue oxygen delivery is critical for survival. Delay in transfusion and antibiotic initiation is uniformly fatal.
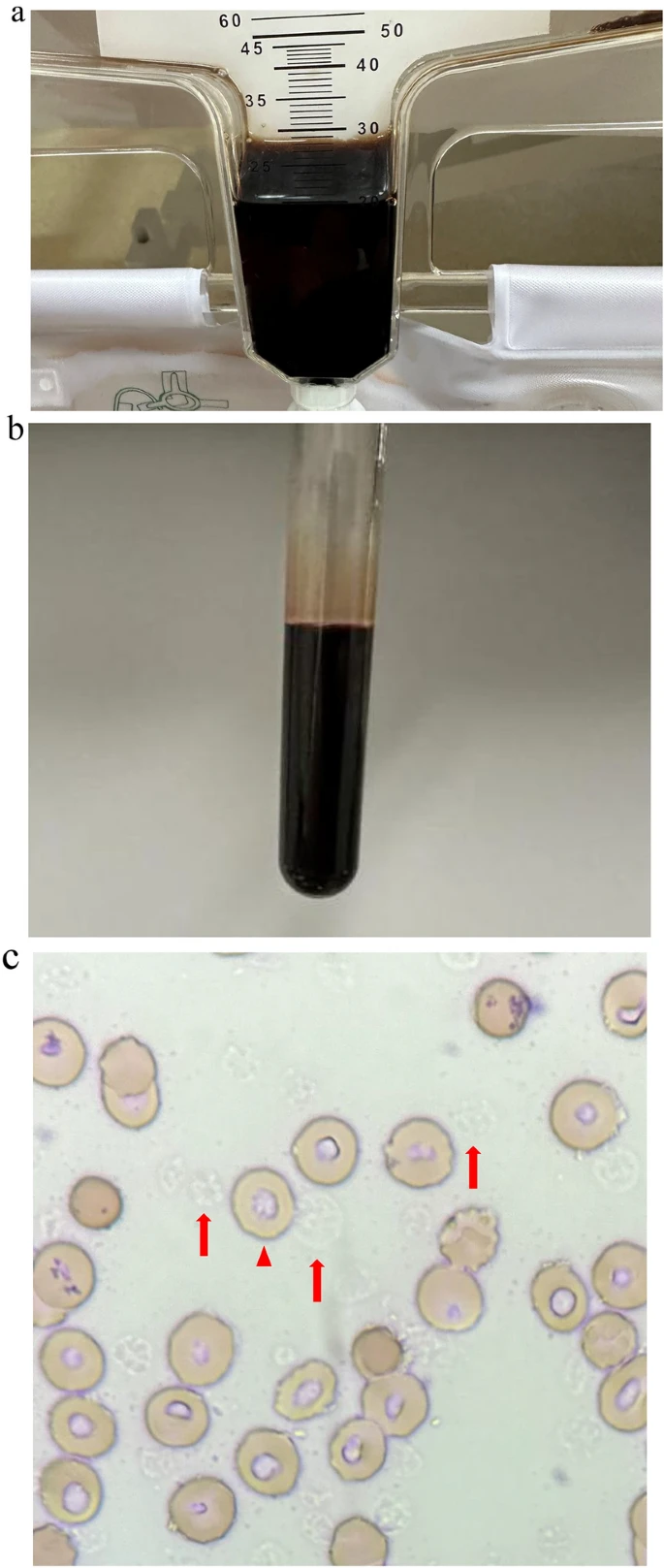
a Reddish-brown urine drained into the indwelling urinary catheter. b Severe in vivo hemolysis prevented separation of cellular components and serum by centrifugation at 3400 revolutions per minute for 7 min. c Peripheral blood smear showing ghost cells (arrows) resulting from dissolution of the erythrocyte membrane and loss of cellular contents due to toxins produced by Clostridium perfringens. The smear was stained with Wright–Giemsa stain and examined under a microscope at ×400 magnification. Arrowheads indicate a normal erythrocyte