Acute respiratory failure unmasking an unexpected disease
Loïc Velten, Anaïs Curtiaud, Antoine Studer, et al
Intensive Care Med (2025). https://doi.org/10.1007/s00134-025-08093-8

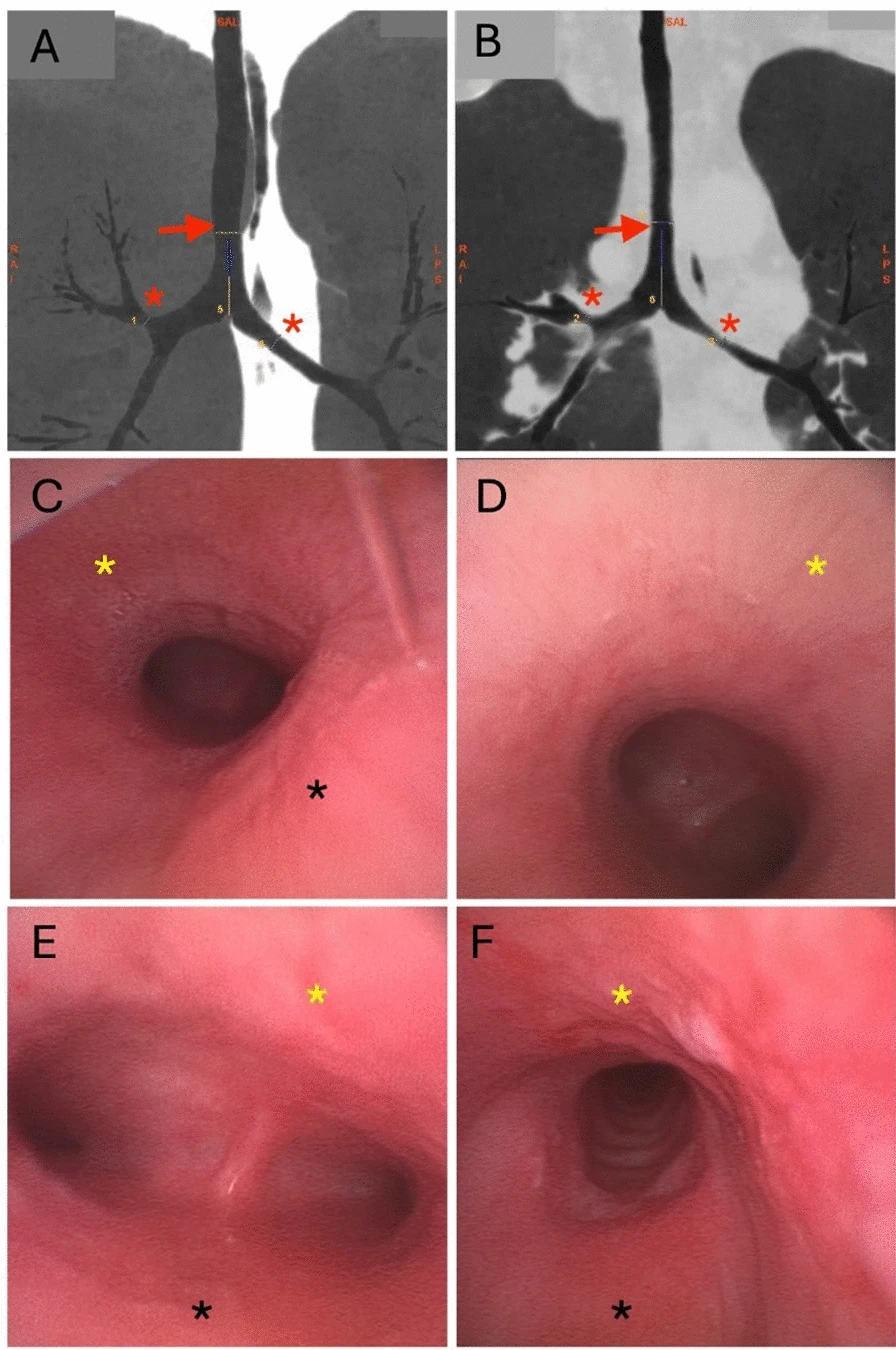
Relapsing polychondritis (RP) is a rare, immune-mediated disease characterized by recurrent inflammation of cartilaginous structures, including the auricles, nasal cartilage, peripheral joints, and respiratory tract (Fig. 1). It affects both men and women, typically presenting around the median age of 50, and is supported, though not definitively confirmed, by histological findings. Airway involvement, affecting the larynx, trachea, and bronchi, occurs in up to half of patients and can be life-threatening. Importantly, respiratory tract manifestations may precede more classic signs such as auricular chondritis or nasal bridge collapse, making early diagnosis challenging for intensivists.
The differential diagnosis includes granulomatosis with polyangiitis (often ANCA-positive with systemic vasculitis), IgG4-related sclerosing disease (the workup for this disease and other rheumatic conditions was negative), COPD (typically showing distal airway obstruction without tracheal cartilage destruction), and other collagen diseases. In addition, recent studies have demonstrated that relapsing polychondritis-like features may occur as part of the clinical spectrum of VEXAS syndrome.
High-dose corticosteroids remain the first-line treatment, often combined with immunosuppressive agents such as cyclophosphamide in severe cases. In this patient, prompt initiation of glucocorticoids and cyclophosphamide allowed weaning from mechanical ventilation and oxygen therapy, as untreated airway inflammation may otherwise progress to irreversible airway collapse.