Carbocisteine or Hypertonic Saline for Acute Respiratory Failure
Bronwen Connolly, Naomi Dickson, Christina Campbell, et al
N Engl J Med Published June 10, 2026
DOI: 10.1056/NEJMoa2603406
Abstract
BACKGROUND
Mucoactive agents are widely used in patients with acute respiratory failure despite limited evidence of their effectiveness or safety.
METHODS
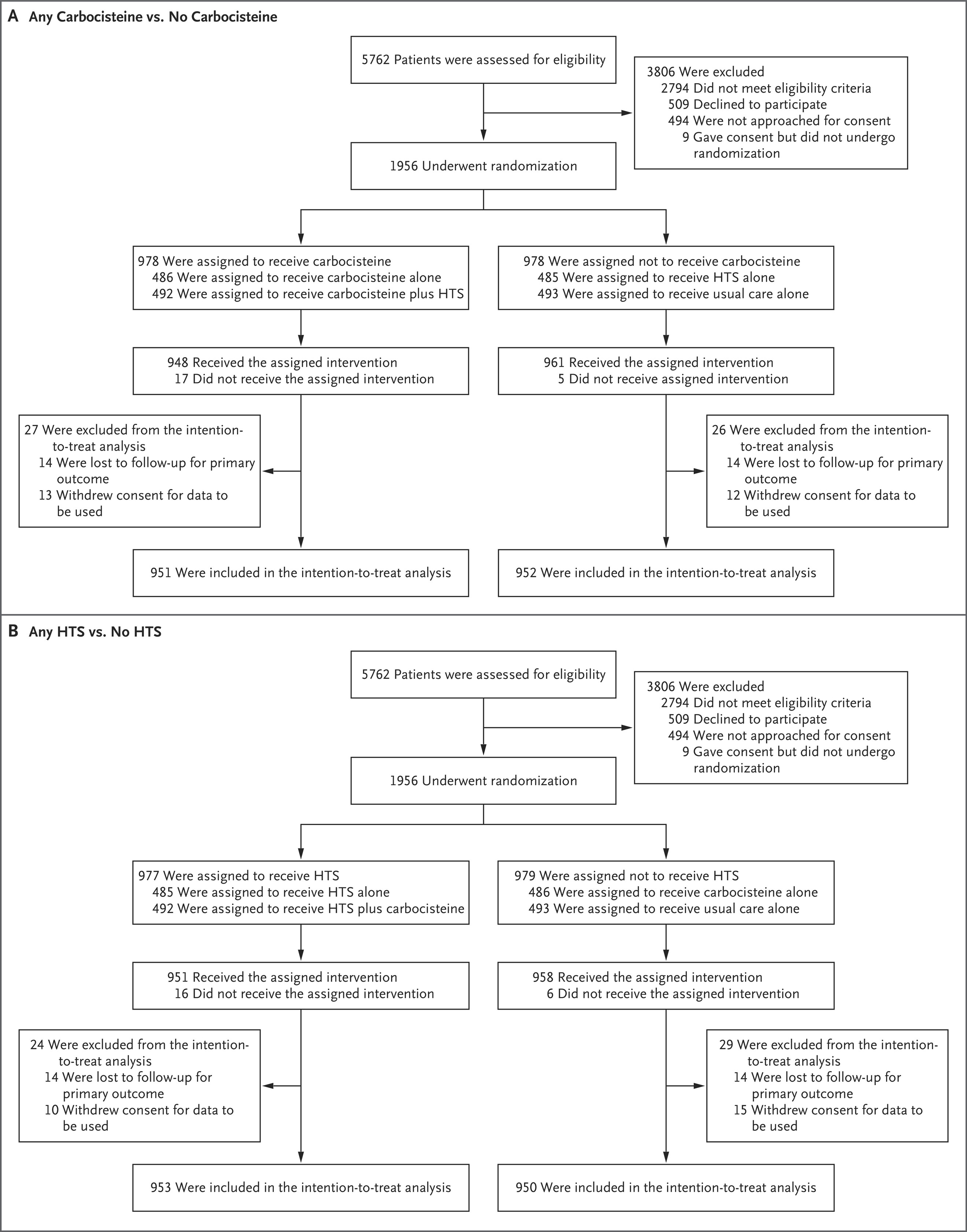
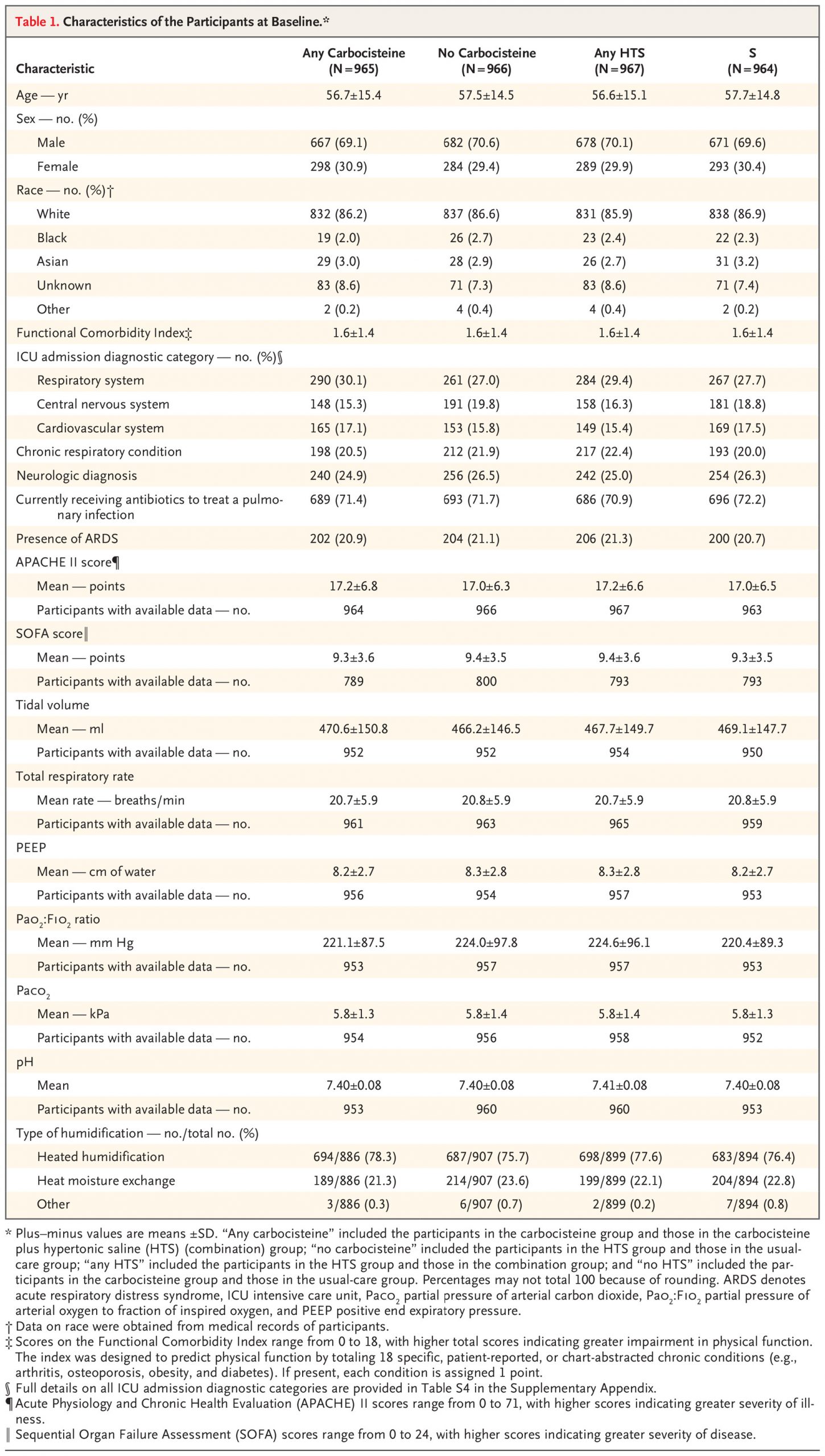
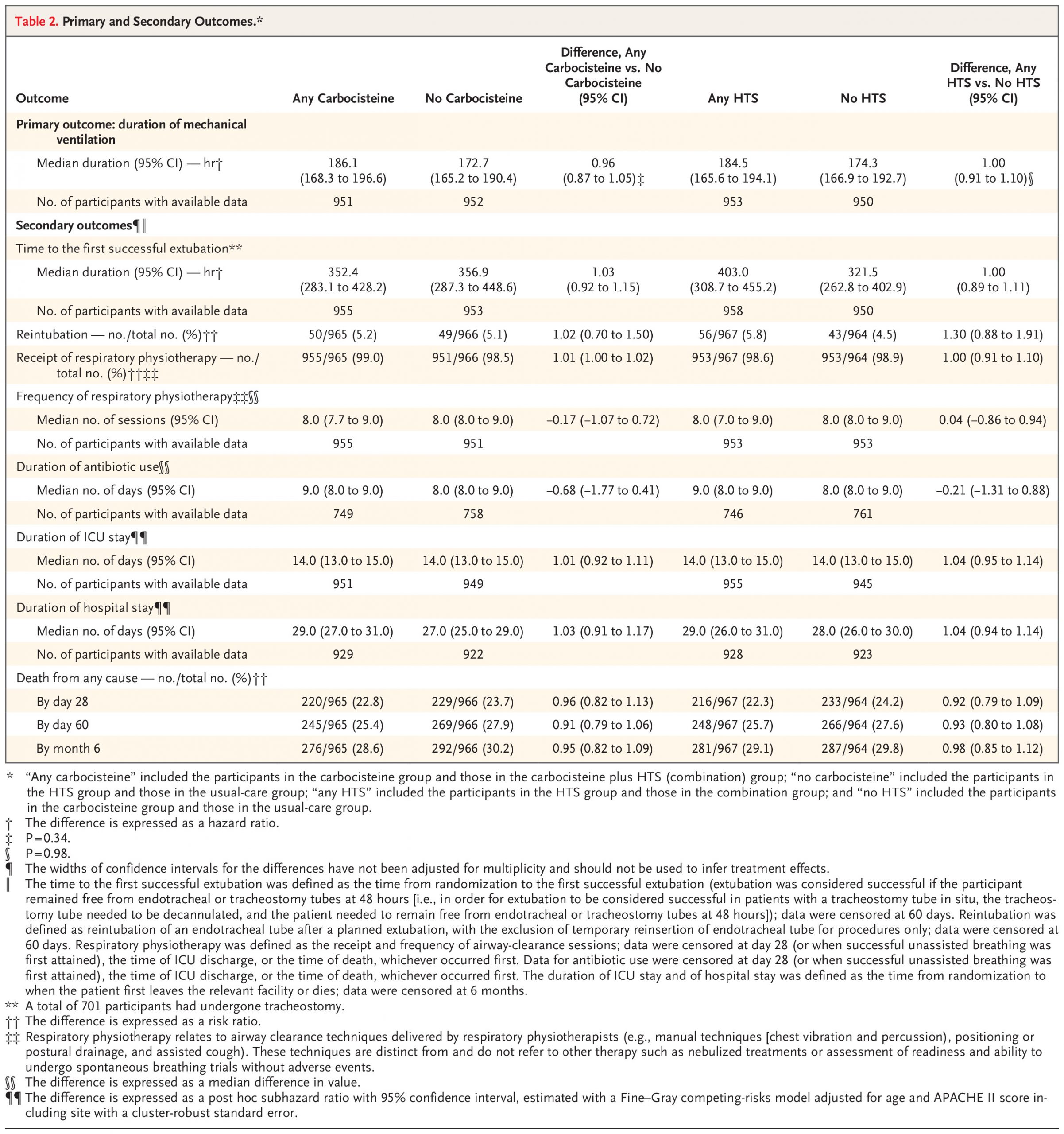
We conducted a multicenter, open-label, randomized trial with a 2-by-2 factorial design that involved critically ill, mechanically ventilated participants 16 years of age or older with acute respiratory failure and difficult-to-clear secretions. All participants received usual care along with carbocisteine (750 mg three times daily enterally), 6% or 7% nebulized hypertonic saline (HTS) (4 ml four times daily), both interventions, or usual care alone for up to 28 days. The primary outcome was duration of mechanical ventilation (from randomization to first successful unassisted breathing). The primary comparisons were between any carbocisteine and no carbocisteine and between any HTS and no HTS, with each comparison comprising two treatment groups.
RESULTS
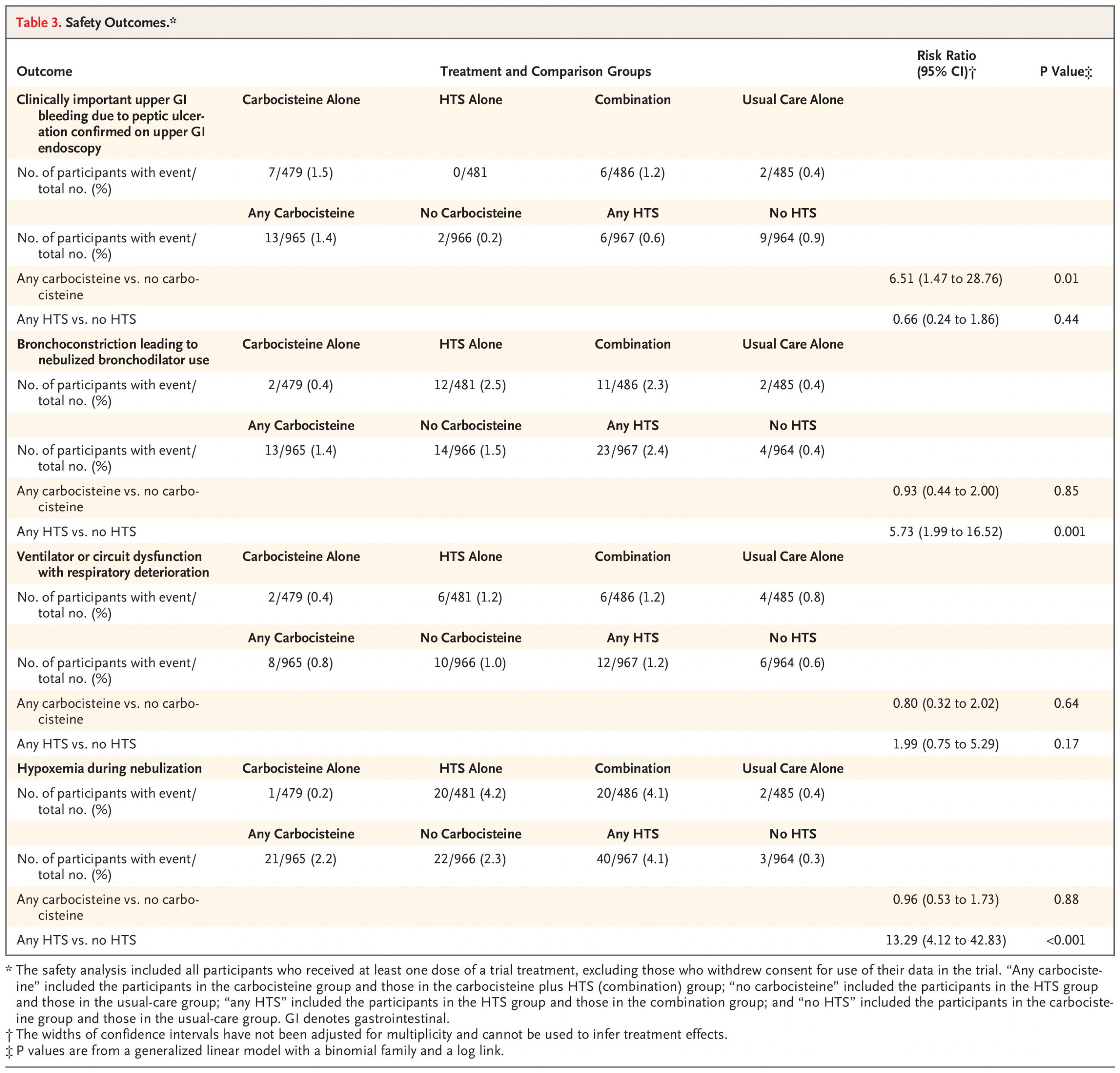
A total of 1956 participants underwent randomization: 486 were assigned to carbocisteine, 485 to HTS, 492 to both treatments, and 493 to usual care alone (472, 474, 479, and 478, respectively, were included in the primary analysis). No evidence of treatment interaction was found (hazard ratio, 1.01, 95% confidence interval [CI], 0.83 to 1.22; P=0.91). The median duration of mechanical ventilation was 186.1 hours (95% CI, 168.3 to 196.6) with carbocisteine and 172.7 hours (95% CI, 165.2 to 190.4) with no carbocisteine (adjusted hazard ratio, 0.96; 95% CI, 0.87 to 1.05; P=0.34) and 184.5 hours (95% CI, 165.6 to 194.1) with HTS and 174.3 hours (95% CI, 166.9 to 192.7) with no HTS (adjusted hazard ratio, 1.00; 95% CI, 0.91 to 1.10; P=0.98). Clinically important upper gastrointestinal bleeding occurred significantly more often with carbocisteine than with no carbocisteine (13 of 965 [1.4%] vs. 2 of 966 [0.2%]; risk ratio, 6.51; 95% CI, 1.47 to 28.76; P=0.01). Bronchoconstriction leading to bronchodilator use occurred significantly more often with HTS than with no HTS (23 of 967 [2.4%] vs. 4 of 964 [0.4%]; risk ratio, 5.73; 95% CI, 1.99 to 16.52; P=0.001), as did hypoxemia during nebulization (40 of 967 [4.1%] vs. 3 of 964 [0.3%]; risk ratio, 13.29; 95% CI, 4.12 to 42.83; P<0.001). One serious adverse reaction was reported in the combination group.
CONCLUSIONS
Among critically ill patients with acute respiratory failure, neither carbocisteine nor HTS significantly reduced the duration of mechanical ventilation, and each was associated with harm. (Funded by the NIHR Health Technology Assessment Programme and the Belfast Health and Social Care Trust Charitable Trust Fund; MARCH ISRCTN Registry number, ISRCTN17683568.)