- Research
- Open access
- Published: 18 July 2024
High flow nasal cannula oxygen therapy versus non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease with acute-moderate hypercapnic respiratory failure: a randomized controlled non-inferiority trial
Dingyu Tan, Bingxia Wang, Peng Cao, et al
Critical Care volume 28, Article number: 250 (2024)
Abstract
Background
Although cumulative studies have demonstrated a beneficial effect of high-flow nasal cannula oxygen (HFNC) in acute hypercapnic respiratory failure, randomized trials to compare HFNC with non-invasive ventilation (NIV) as initial treatment in acute exacerbations of chronic obstructive pulmonary disease (AECOPD) patients with acute-moderate hypercapnic respiratory failure are limited. The aim of this randomized, open label, non-inferiority trial was to compare treatment failure rates between HFNC and NIV in such patients.
Methods
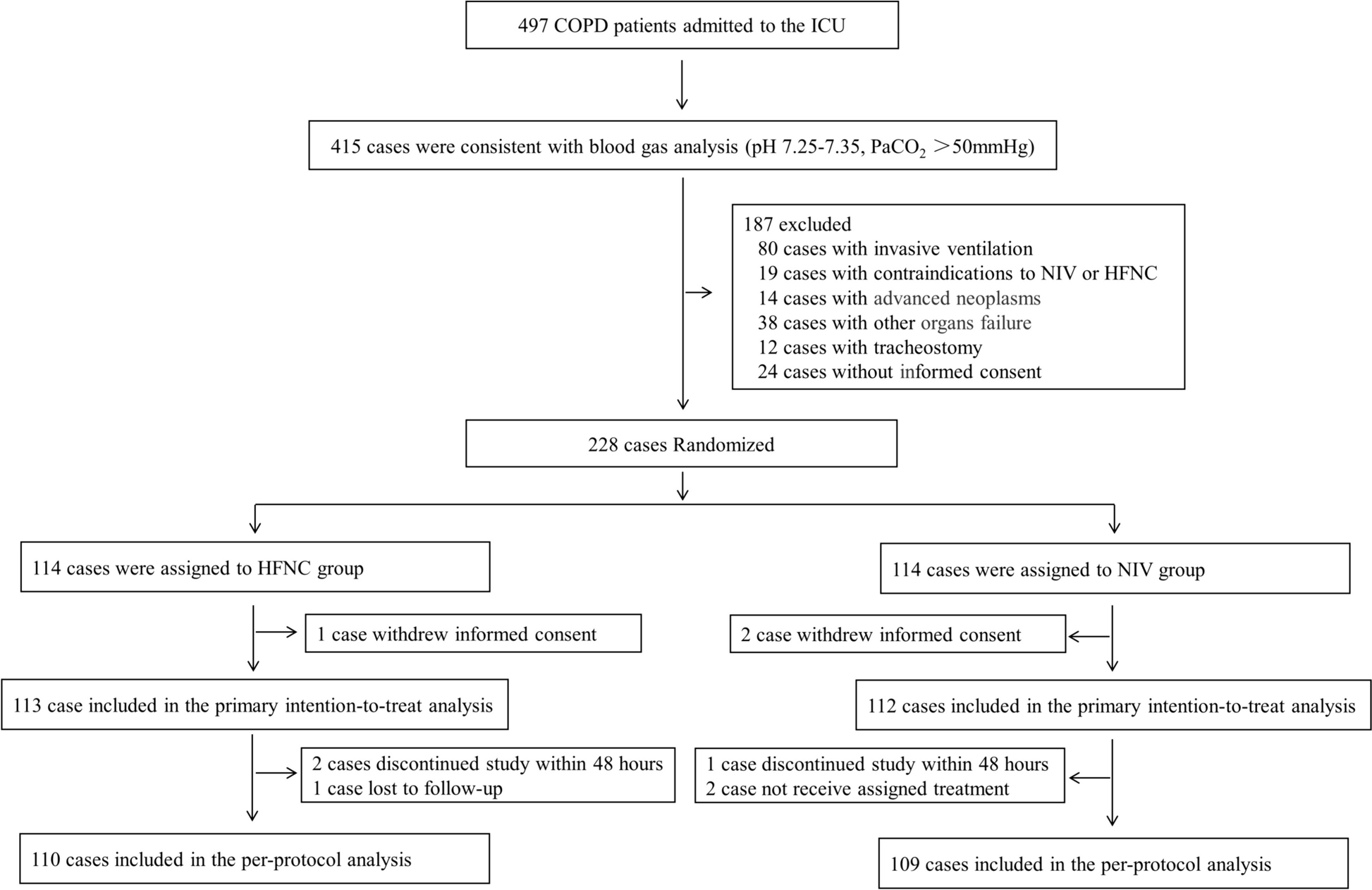
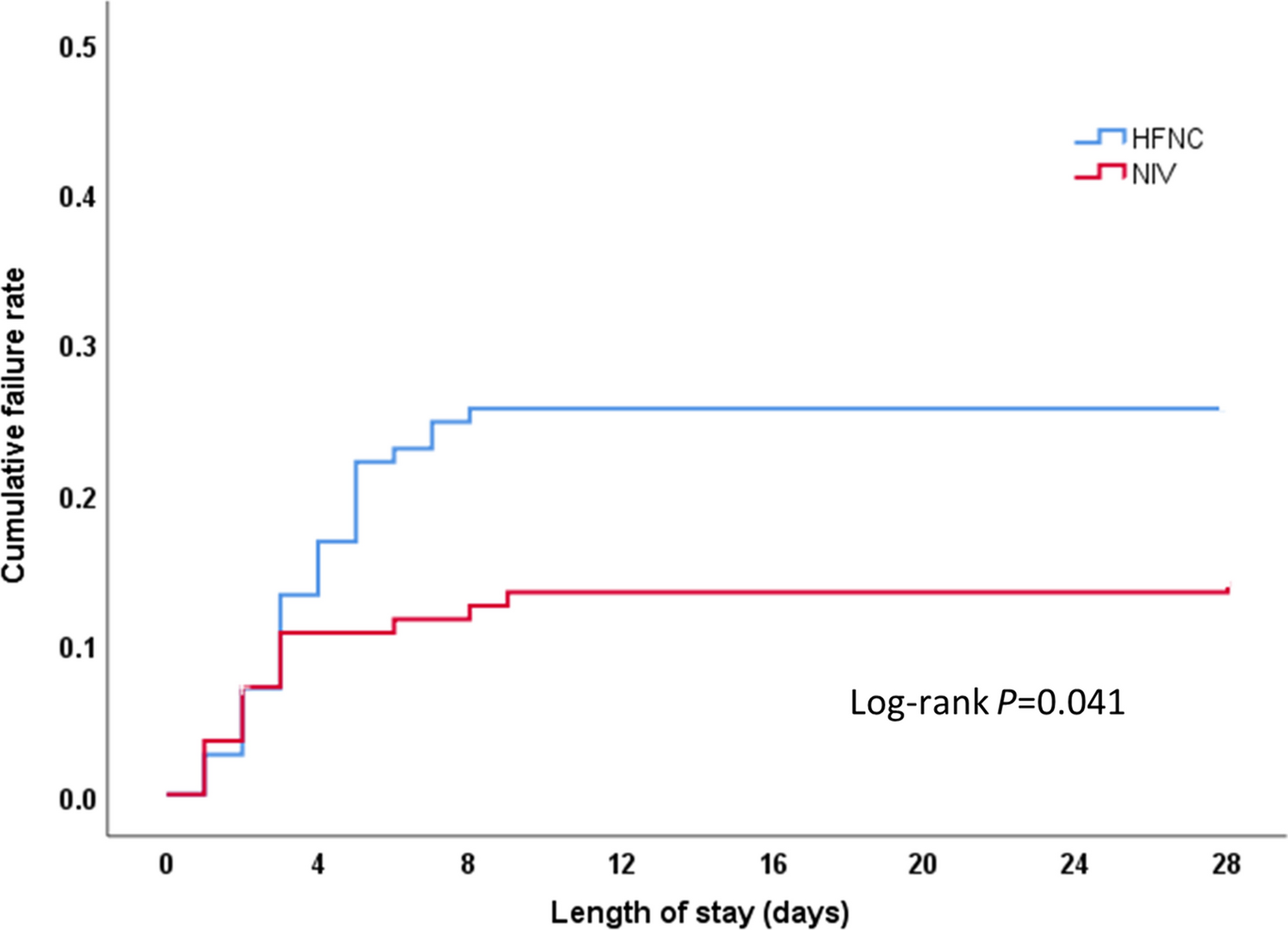
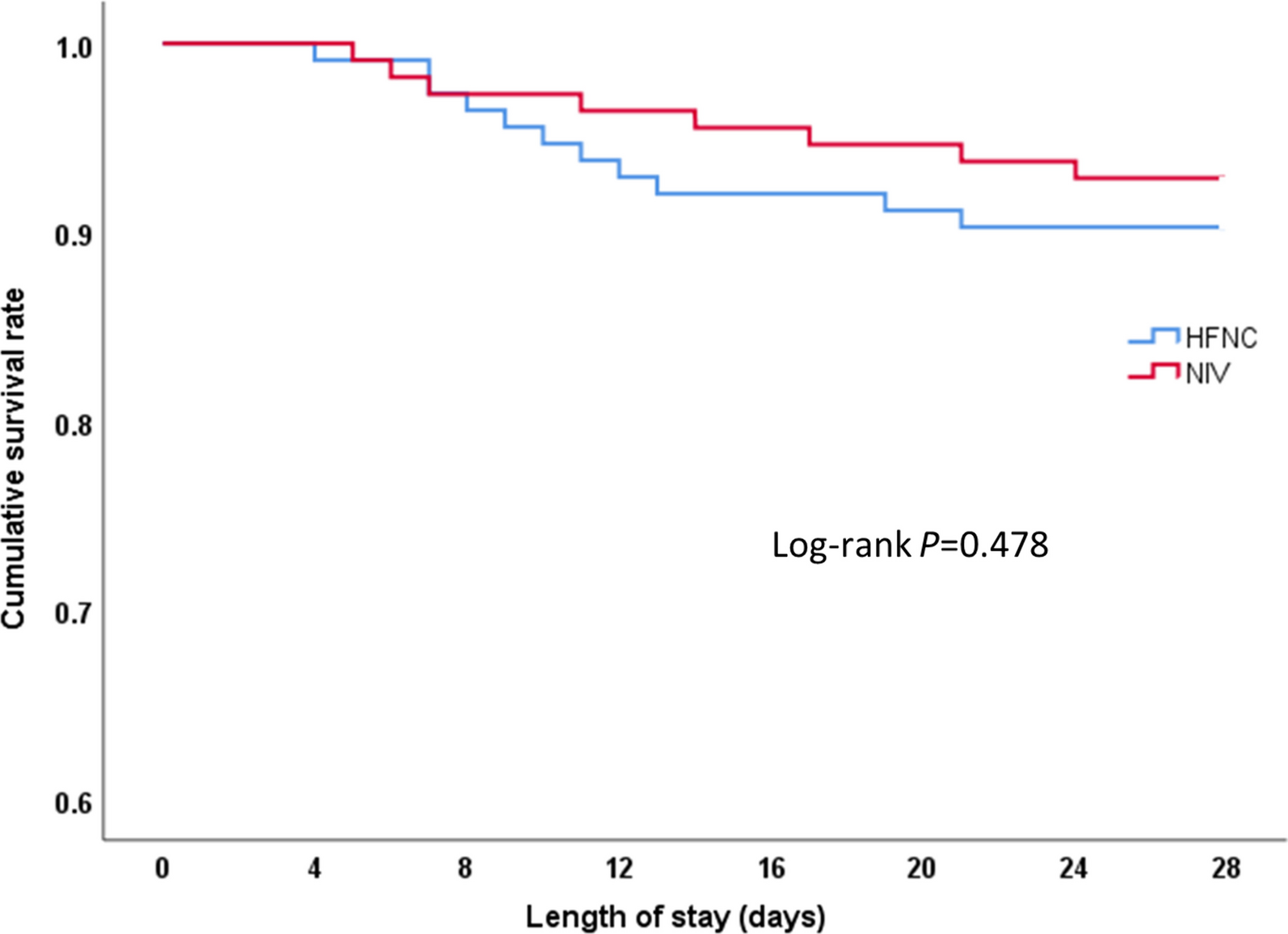
Patients diagnosed with AECOPD with a baseline arterial blood gas pH between 7.25 and 7.35 and PaCO2 ≥ 50 mmHg admitted to two intensive care units (ICUs) at a large tertiary academic teaching hospital between March 2018 and December 2022 were randomly assigned to HFNC or NIV. The primary endpoint was the rate of treatment failure, defined as endotracheal intubation or a switch to the other study treatment modality. Secondary endpoints were rates of intubation or treatment change, blood gas values, vital signs at one, 12, and 48 h, 28-day mortality, as well as ICU and hospital lengths of stay.
Results
225 total patients (113 in the HFNC group and 112 in the NIV group) were included in the intention-to-treat analysis. The failure rate of the HFNC group was 25.7%, while the NIV group was 14.3%. The failure rate risk difference between the two groups was 11.38% (95% CI 0.25–21.20, P = 0.033), which was higher than the non-inferiority cut-off of 9%. In the per-protocol analysis, treatment failure occurred in 28 of 110 patients (25.5%) in the HFNC group and 15 of 109 patients (13.8%) in the NIV group (risk difference, 11.69%; 95% CI 0.48–22.60). The intubation rate in the HFNC group was higher than in the NIV group (14.2% vs 5.4%, P = 0.026). The treatment switch rate, ICU and hospital length of stay or 28-day mortality in the HFNC group were not statistically different from the NIV group (all P > 0.05).
Conclusion
HFNC was not shown to be non-inferior to NIV and resulted in a higher incidence of treatment failure than NIV when used as the initial respiratory support for AECOPD patients with acute-moderate hypercapnic respiratory failure.
Trial registration: chictr.org (ChiCTR1800014553). Registered 21 January 2018, http://www.chictr.org.cn