Monocyte HLA-DR expression in septic shock patients: insights from a 20-year real-world cohort of 1023 cases
Monneret G, Lafon T, Gossez M, et al.
Intensive Care Med(2025). https://doi.org/10.1007/s00134-025-08110-w
Abstract
Purpose
Septic patients simultaneously experience hyperinflammation and immunosuppression, the latter driving ICU-acquired infections, prolonged stays in ICU, and increased mortality. As immunostimulant therapies enter clinical trials, effective stratification is critical to identify patients with the most profound immune dysfunction. Monocyte HLA-DR expression (mHLA-DR) has emerged as the most reliable and actionable biomarker of sepsis-induced immunosuppression.
Methods
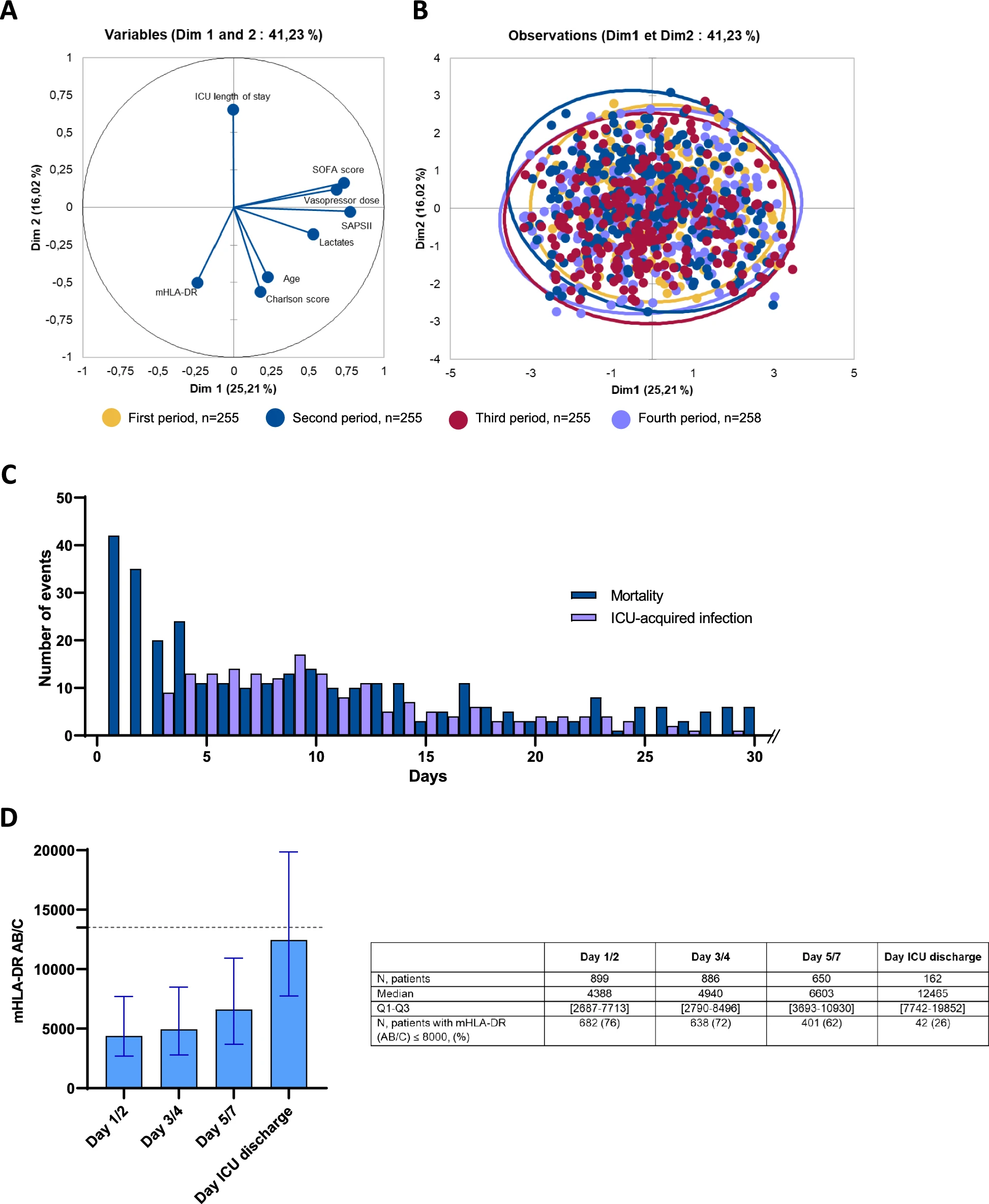
We conducted a real-world, 20-year cohort study of 1023 septic shock patients, measuring mHLA-DR by standardized flow cytometry during the first week of ICU admission. Primary outcomes included day-28 and day-90 mortality, and ICU-acquired infections.
Results
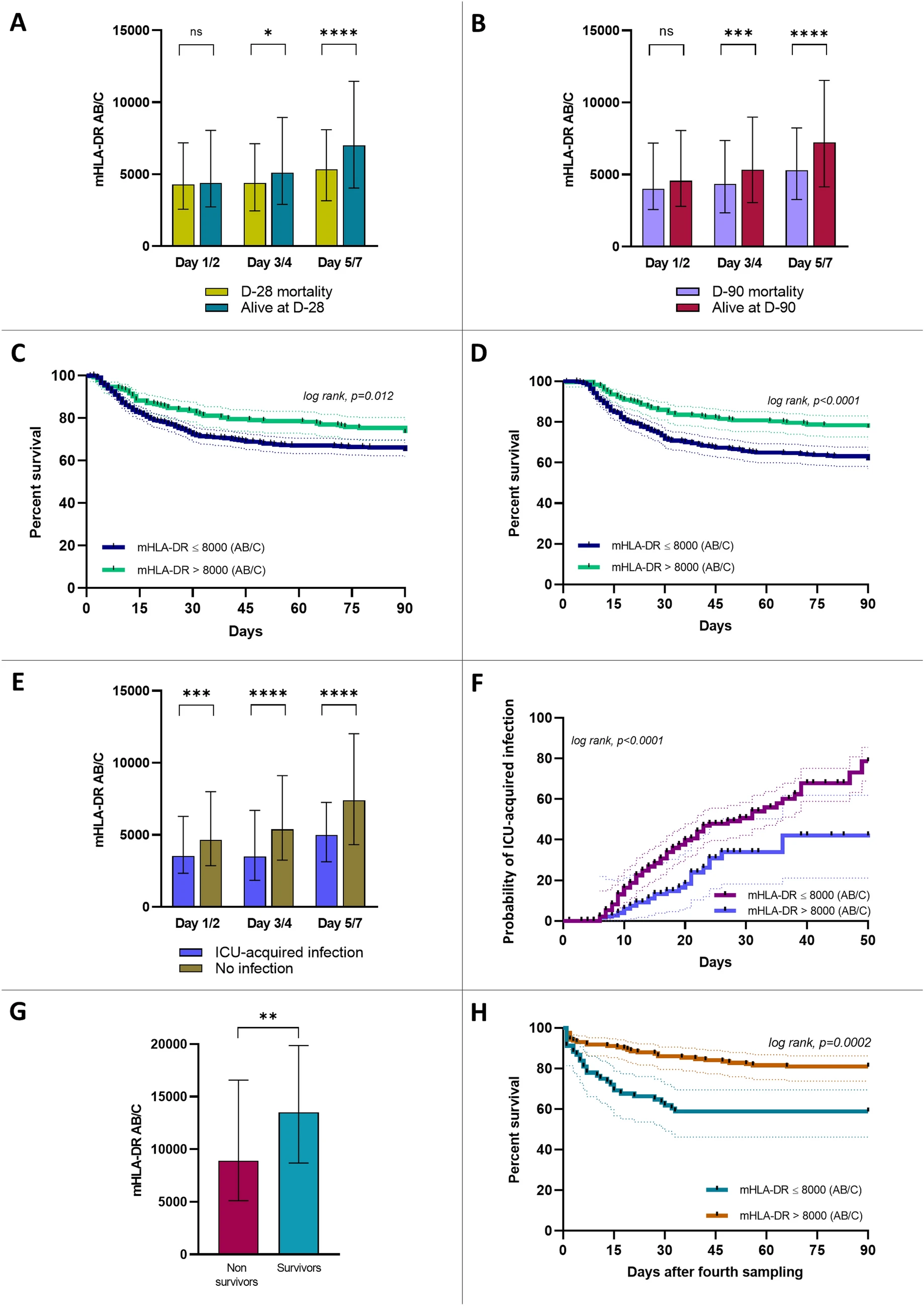
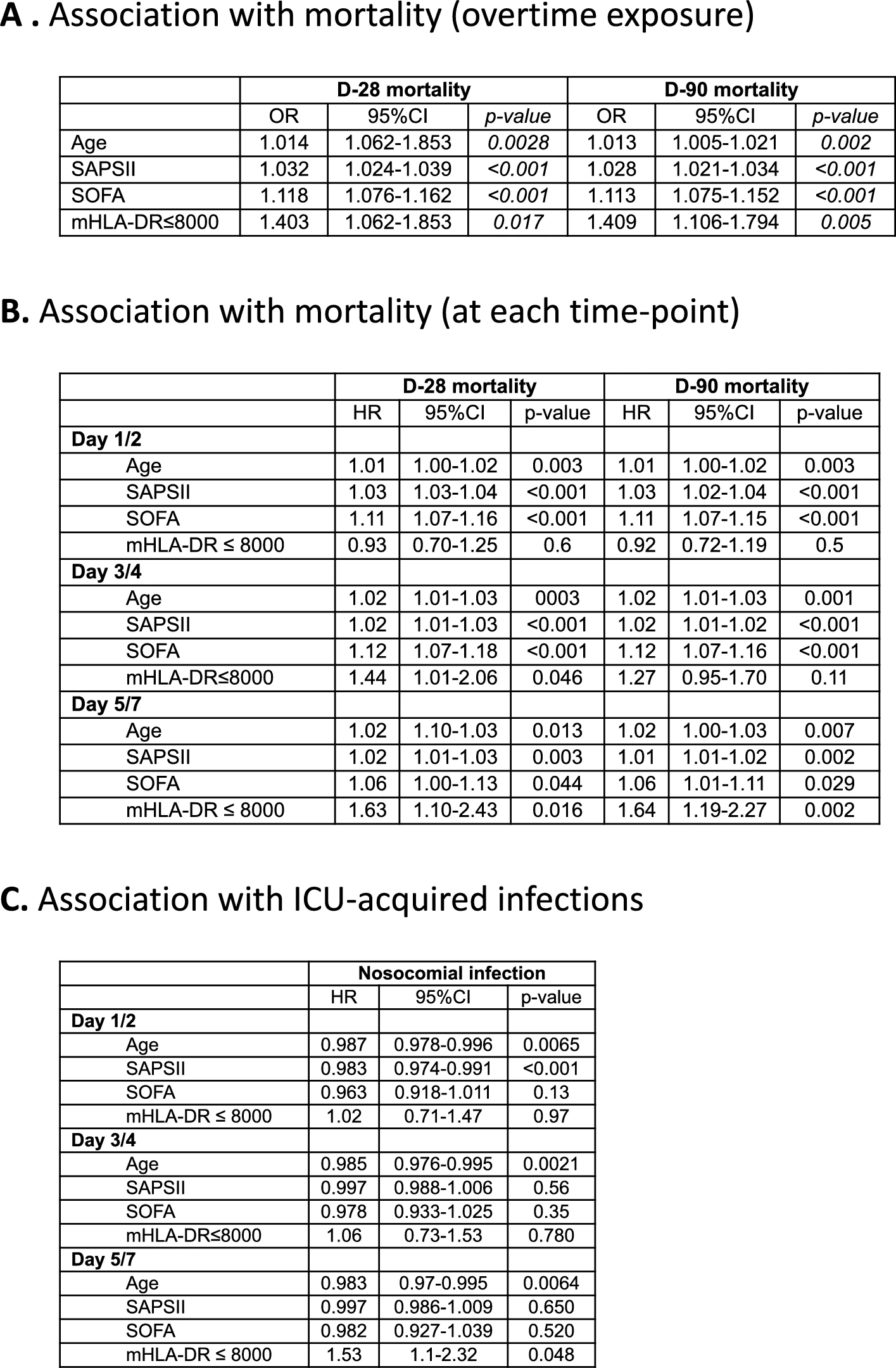
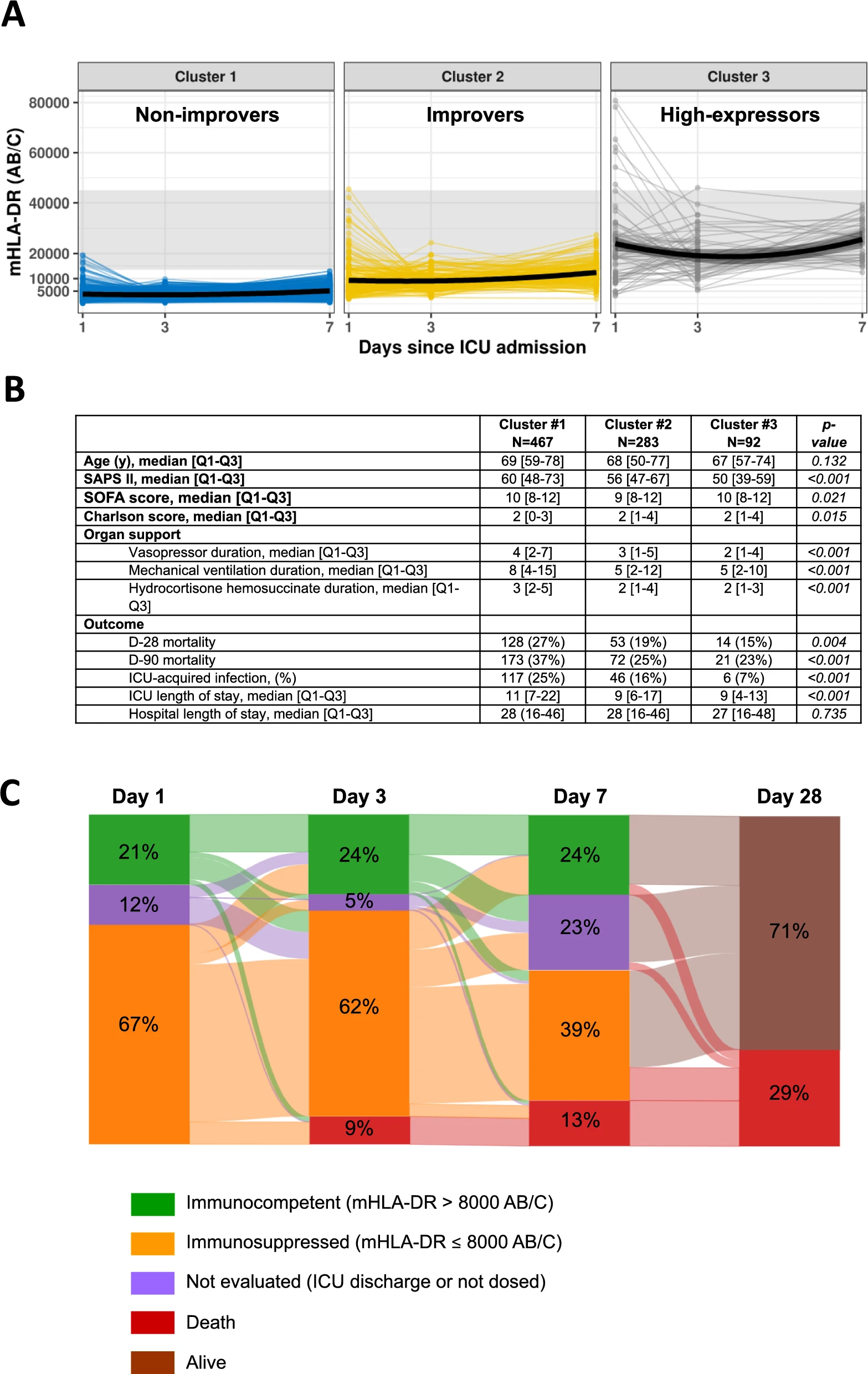
Low mHLA-DR (< 8000 AB/C, a threshold already used in phase II trials) was significantly associated with increased mortality and ICU-acquired infections. This association held across static and dynamic measures, multivariate analyses, Kaplan–Meier survival curves, and trajectory clustering (K-means).
Conclusions
This large real-world study confirms that mHLA-DR is a robust enrichment biomarker for identifying the most immunosuppressed septic shock patients at higher risk of adverse outcomes. Importantly, time-course analysis suggests that early immune downregulation may represent a physiological adaptation, while delayed and persistent immunosuppression is associated with worse outcomes. Early single time-point measurements may fail to identify patients who are unlikely to develop delayed immunosuppression. Tracking mHLA-DR trajectories after the initial ICU days is essential for detecting persistent immune dysfunction and selecting patients in case of immunostimulant approaches.