Imaging in Intensive Care Medicine
Serum sickness: a mimic of septic shock
Takafumi Todaka
Intensive Care Med Published: 17 September 2025
https://doi.org/10.1007/s00134-025-08118-2
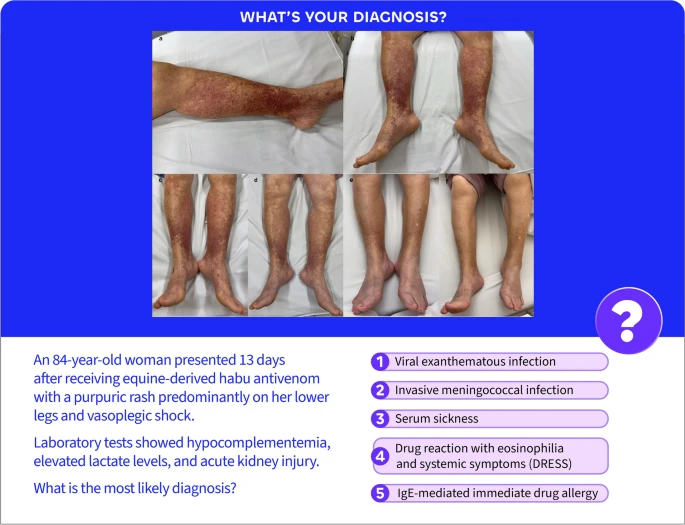
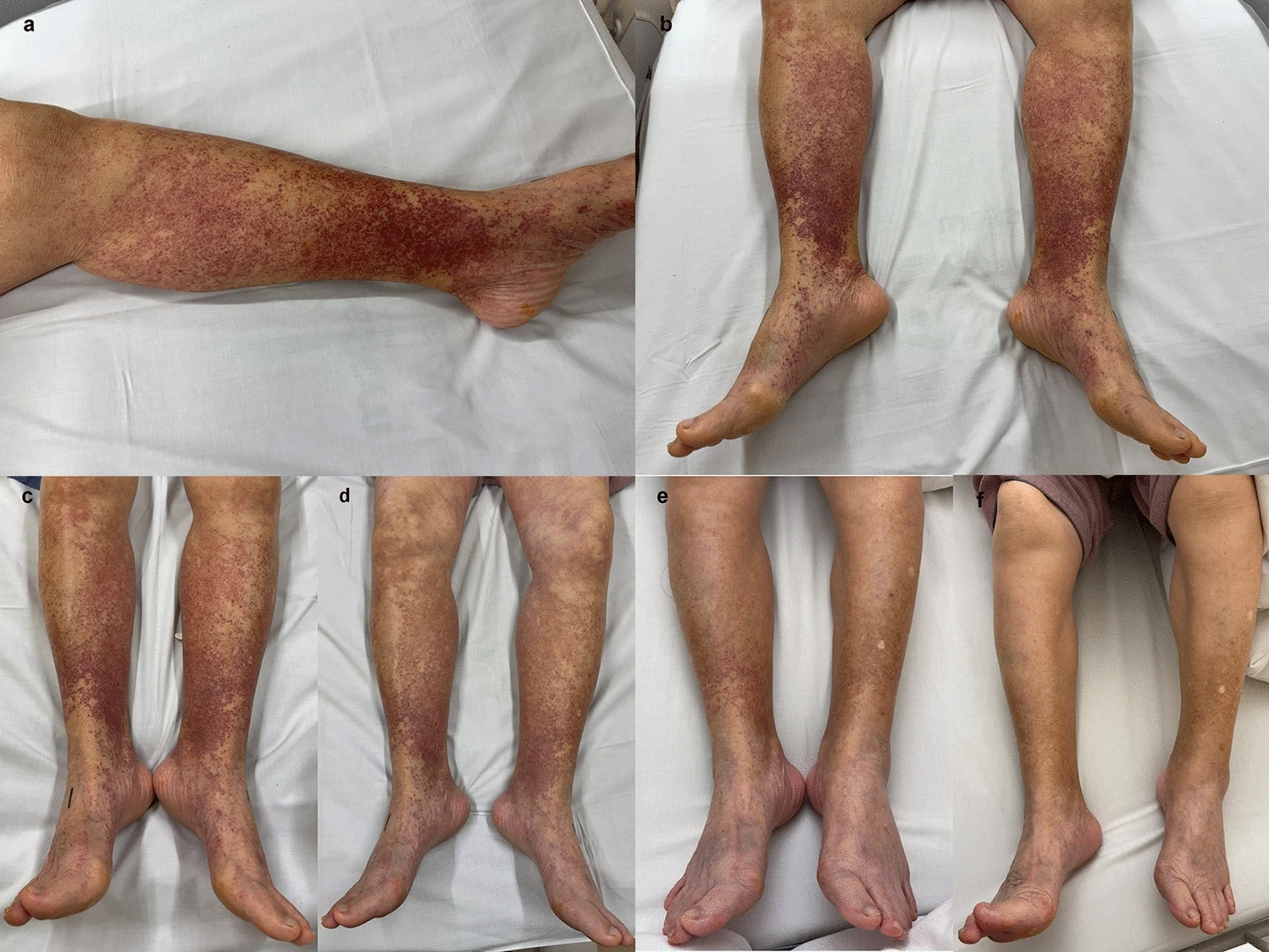
Serum sickness typically manifests 7–14 days after exposure to heterologous proteins, such as antivenoms, some vaccines, and immune-modulating agents (e.g., rituximab and infliximab). Most cases resolve with withdrawal of the offending agent; however, severe systemic involvement may require corticosteroids. Purpuric lesions together with hypotension, tachypnea, and elevated lactate can also raise concern for invasive pneumococcal or meningococcal infection. Accordingly, septic shock ranked high in the differential, and empiric meropenem was initiated. It is a diagnostic challenge to distinguish serum sickness from sepsis (Fig. 1).
Serum sickness is an immune complex-mediated type III reaction that typically presents 7–14 days after exposure to heterologous proteins, most commonly snake antivenoms, some vaccines, and immune- and cell-metabolism modulators, such as rituximab and infliximab. As rituximab and infliximab are widely used monoclonal antibodies, intensivists may occasionally manage critically ill patients with serum sickness after treatment with these agents.
Clinical features. The most common findings are pruritic rash, fever, malaise, and polyarthralgia. The rash is heterogeneous, including urticarial, morbilliform, maculopapular, or palpable purpura. The mucous membranes are typically spared. In severe cases, laboratory tests show hypocomplementemia, with low C3, C4, and CH50 levels, reflecting complement consumption.
Differential diagnosis. Rash with shock: treat as an infectious emergency, especially for invasive meningococcal infection. Resuscitation and evaluation should be initiated concurrently, and local infection control precautions should be followed.
Management. The prognosis is generally excellent; once further exposure is avoided, most patients recover within days to weeks without scarring or lasting sequelae. In the ICU, resuscitation and hemodynamic support should be prioritized. When systemic involvement is significant, a short course of systemic corticosteroids may be used (e.g., hydrocortisone IV 200 mg/day, followed by oral prednisone/prednisolone with a 5–7-day taper guided by clinical response). Stop and avoid further exposure to the culprit antigen, document the product, and counsel against re-exposure, as subsequent exposure may precipitate anaphylaxis.