Combined use of a multiplex PCR and serum procalcitonin to reduce antibiotic exposure in critically ill patients with community-acquired pneumonia: the MULTI-CAP randomized controlled trial
Voiriot, G., Argaud, L., Cohen, Y. et al.
Intensive Care Med(2025). https://doi.org/10.1007/s00134-025-08014-9
Abstract
Purpose
Multiplex polymerase chain reaction (mPCR) testing has the potential to rapidly and accurately identify causative microorganisms in patients with community-acquired pneumonia (CAP). Its use in a management strategy, along with biomarkers, may reduce antibiotic exposure and improve clinical outcomes.
Methods
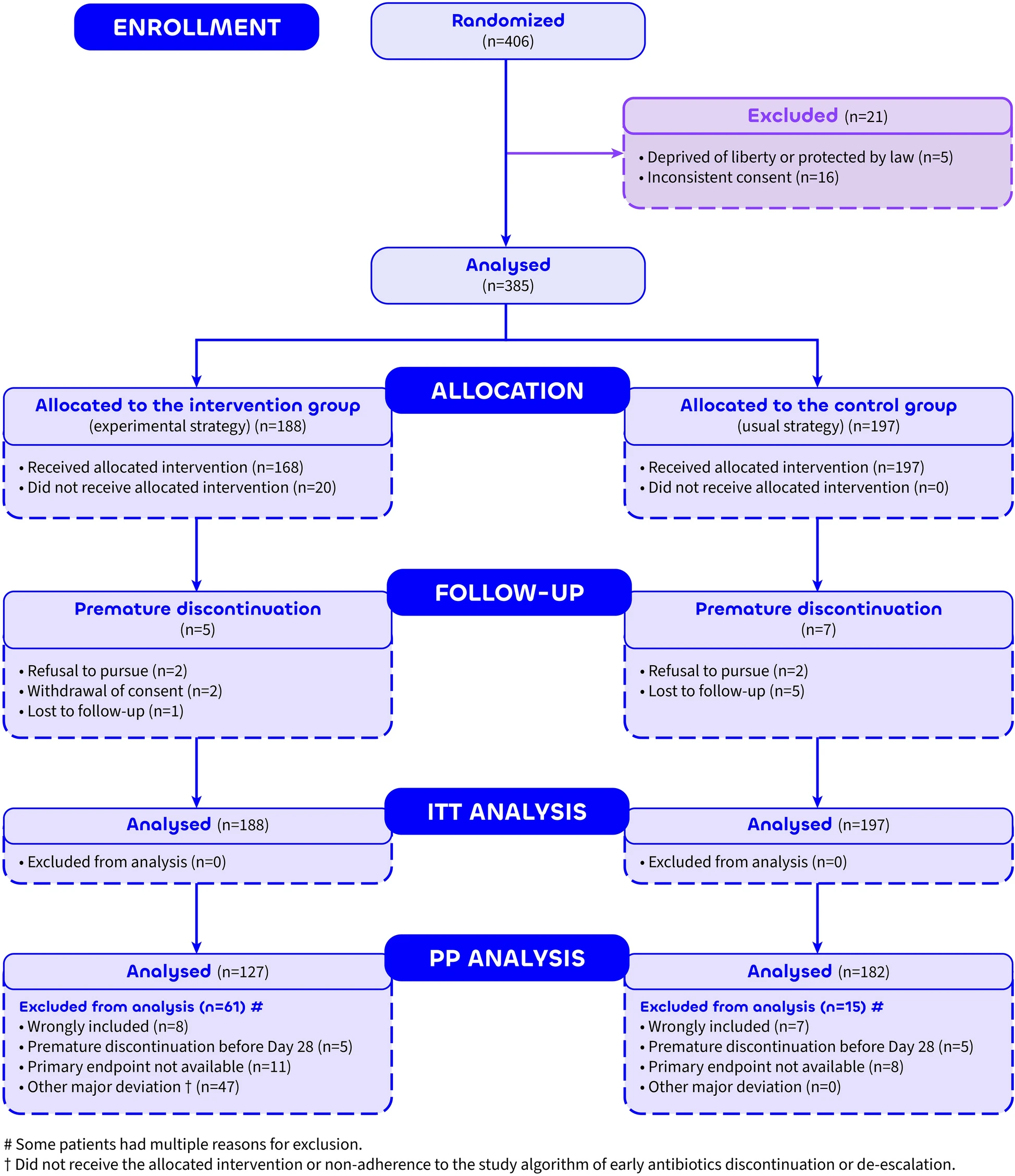
The MULTI-CAP trial was a multicenter (n = 20), parallel-group, superiority, open-label, randomized trial. Subjects were non-immunocompromised adult patients (≥ 18 years) admitted to the intensive care unit (ICU) for CAP and randomly assigned in a 1:1 ratio. In the intervention group, the microbiological diagnosis combined a broad-spectrum respiratory mPCR and conventional microbiological investigations. An algorithm for early discontinuation or de-escalation of antibiotics was applied, based on mPCR results and serum procalcitonin. In the control group, only conventional microbiological investigations were performed. In both groups, antibiotic discontinuation was considered on Day 3 and day after day until Day 7, based on procalcitonin values and kinetics. The primary endpoint was defined as the number of days alive without any antibiotic from the time of enrollment to Day 28.
Results
From October 4, 2018, to March 3, 2022, 406 patients were randomized, and 385 were evaluable in the intention-to-treat analysis. The median number of days alive without antibiotics on Day 28 was 19.0 (0.0; 24.0) days in the intervention group and 19.0 (7.0; 22.0) days in the control group (difference, 0.0 (95% CI, − 4.0 to 4.0). However, the antibiotic cumulative duration on day 28 was 3 days shorter (95% CI, − 5.1 to − 0.9) in the intervention group. Serious adverse events did not differ between groups.


Conclusion
In ICU patients with CAP, a management strategy combining a mPCR and serum procalcitonin failed to reduce antibiotic exposure or improve outcomes on Day 28, compared to usual care.
Trial registration number
NCT03452826 (March 2018), EudraCT 2017-A01615-48.