ORIGINAL ARTICLE
Levosimendan for Hemodynamic Support after Cardiac Surgery
Giovanni Landoni, Vladimir V. Lomivorotov, Gabriele Alvaro, et al.
BACKGROUND 背景
Acute left ventricular dysfunction is a major complication of cardiac surgery and is associated with increased mortality. Meta-analyses of small trials suggest that levosimendan may result in a higher rate of survival among patients undergoing cardiac surgery.
急性左心室功能不全是心脏术后的主要并发症,伴随病死率升高。小样本研究的meta分析提示,左西孟旦能够提高心脏外科手术患者的生存率。
METHODS 方法
We conducted a multicenter, randomized, double-blind, placebo-controlled trial involving patients in whom perioperative hemodynamic support was indicated after cardiac surgery, according to prespecified criteria. Patients were randomly assigned to receive levosimendan (in a continuous infusion at a dose of 0.025 to 0.2 μg per kilogram of body weight per minute) or placebo, for up to 48 hours or until discharge from the intensive care unit (ICU), in addition to standard care. The primary outcome was 30-day mortality.
我们进行了一项多中心、随机、安慰剂对照试验,入选根据事前确定的标准在心脏术后接受围手术期血流动力学支持治疗的患者。除标准治疗外,患者被随机分为左西孟旦组(持续输注0.025 - 0.2 μg/kg/min)或安慰剂组,治疗持续48小时或直至从ICU转出。主要预后指标为30天病死率。
RESULTS 结果
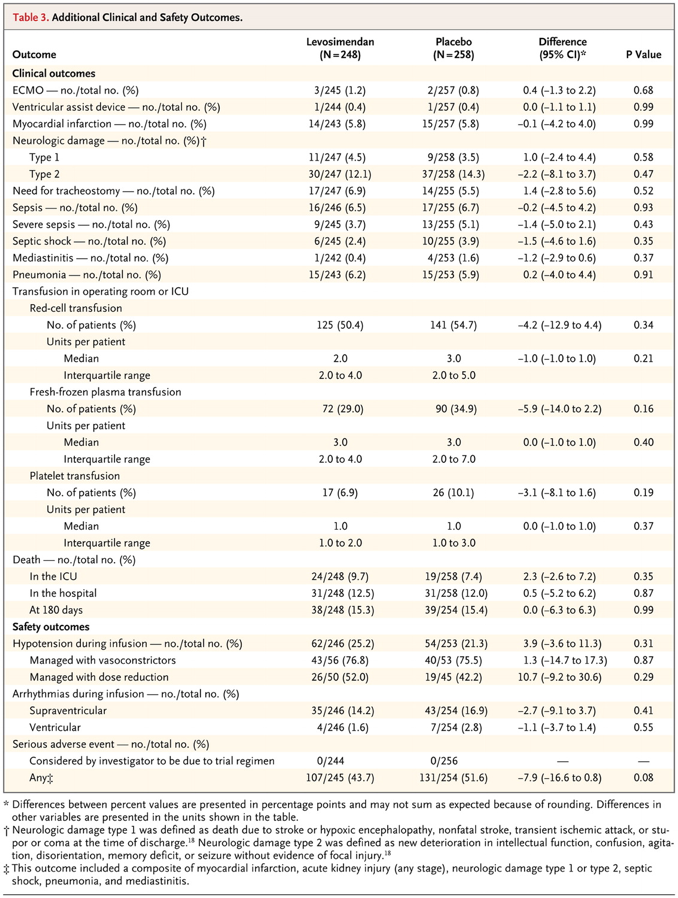
The trial was stopped for futility after 506 patients were enrolled. A total of 248 patients were assigned to receive levosimendan and 258 to receive placebo. There was no significant difference in 30-day mortality between the levosimendan group and the placebo group (32 patients [12.9%] and 33 patients [12.8%], respectively; absolute risk difference, 0.1 percentage points; 95% confidence interval [CI], −5.7 to 5.9; P=0.97). There were no significant differences between the levosimendan group and the placebo group in the durations of mechanical ventilation (median, 19 hours and 21 hours, respectively; median difference, −2 hours; 95% CI, −5 to 1; P=0.48), ICU stay (median, 72 hours and 84 hours, respectively; median difference, −12 hours; 95% CI, −21 to 2; P=0.09), and hospital stay (median, 14 days and 14 days, respectively; median difference, 0 days; 95% CI, −1 to 2; P=0.39). There was no significant difference between the levosimendan group and the placebo group in rates of hypotension or cardiac arrhythmias.
在入选506名患者后,因治疗无效,研究提前终止。共有248名患者被分配接受左西孟旦治疗,258名患者使用安慰剂。左西孟旦组与安慰剂组30天病死率无显著差异(分别为32 名患者 [12.9%] 及 33 名患者 [12.8%];绝对风险差异,0.1%; 95% 可信区间 [CI], −5.7 to 5.9; P=0.97)。两组患者机械通气时间(中位数分别为 19 和 21 小时;中位数差异−2 小时; 95% CI, −5 to 1; P=0.48),ICU住院日(中位数分别为72 和 84 小时;中位数差异−12 小时;95% CI, −21 to 2; P=0.09)及总住院日(中位数分别为 14 和 14 天;中位数差异 0 天;95% CI, −1 to 2; P=0.39)均无显著差异。左西孟旦组与安慰剂组低血压或心律失常的发生率无显著差异。




CONCLUSIONS 结论
In patients who required perioperative hemodynamic support after cardiac surgery, low-dose levosimendan in addition to standard care did not result in lower 30-day mortality than placebo.
对于心脏术后需要围手术期血流动力学支持治疗的患者而言,在常规治疗的基础上加用小剂量左西孟旦不能降低30天病死率。
(Funded by the Italian Ministry of Health; CHEETAH ClinicalTrials.gov number, NCT00994825.)